. I saw her at her 3 mont_1.jpg)


Distal Humerus Nonunion with Segmental Bone Loss and Autograft Reconstruction.
Score and Comment on this Case
Clinical Details
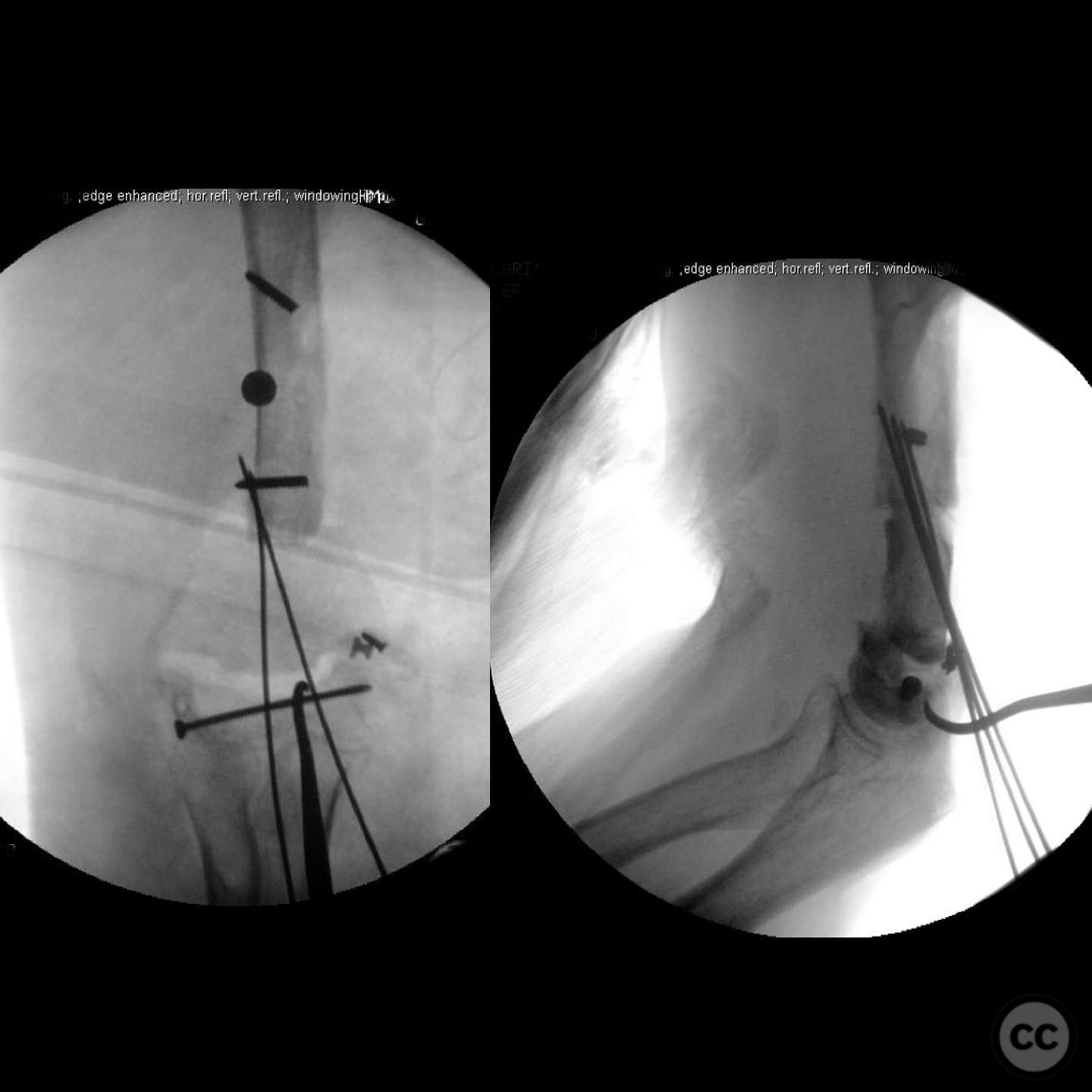
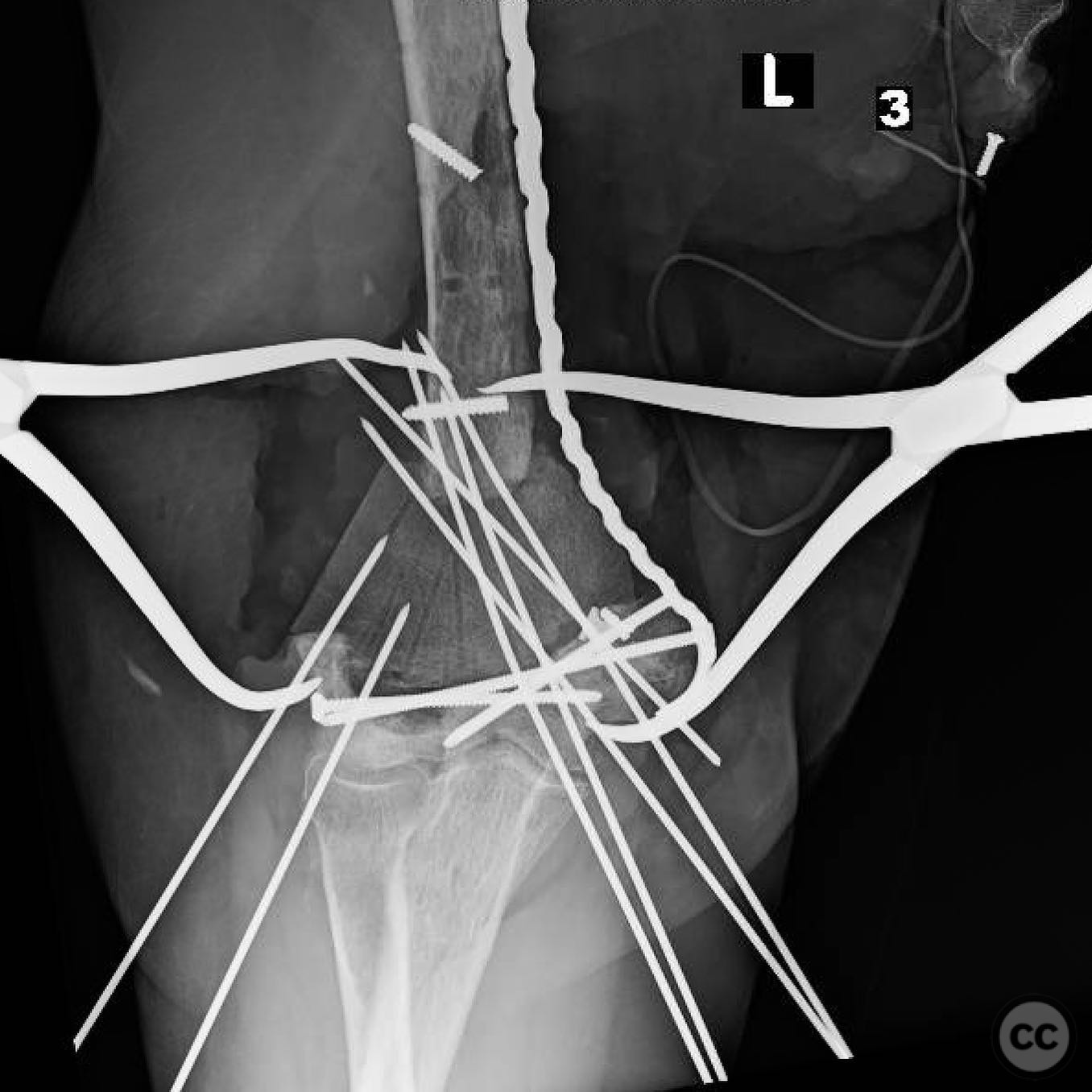
Clinical and radiological findings: A 60-year-old female patient, with a history of obesity, presented with a distal humerus nonunion and segmental bone loss following a supracondylar intercondylar fracture initially treated in 2016. The patient had been lost to follow-up until 2020, when she reported persistent elbow pain, grinding, and swelling. The fracture was initially closed, with uneventful wound healing and no signs of infection. The affected limb is the non-dominant arm. Radiological assessment confirmed the presence of nonunion with segmental bone loss.
Preoperative Plan
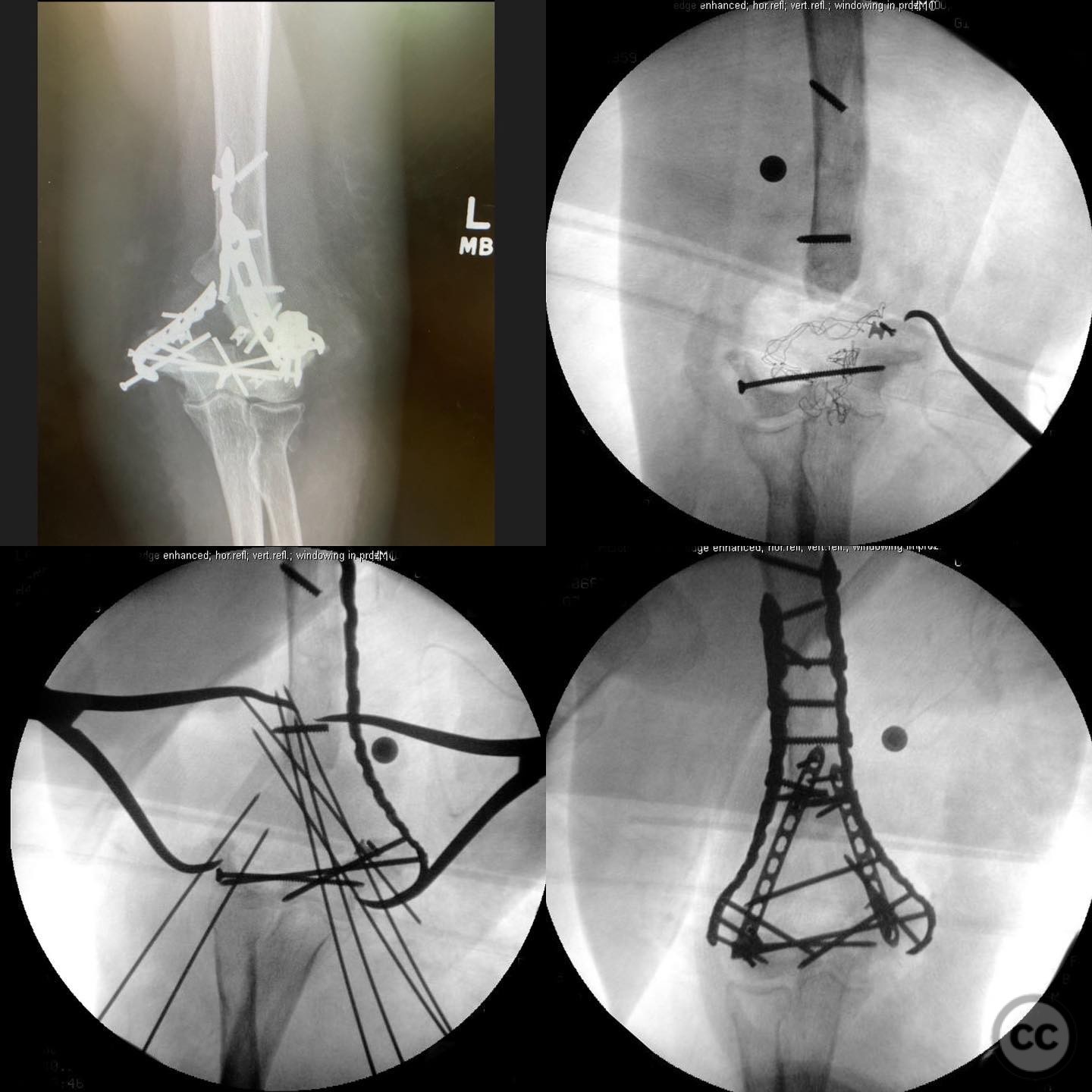
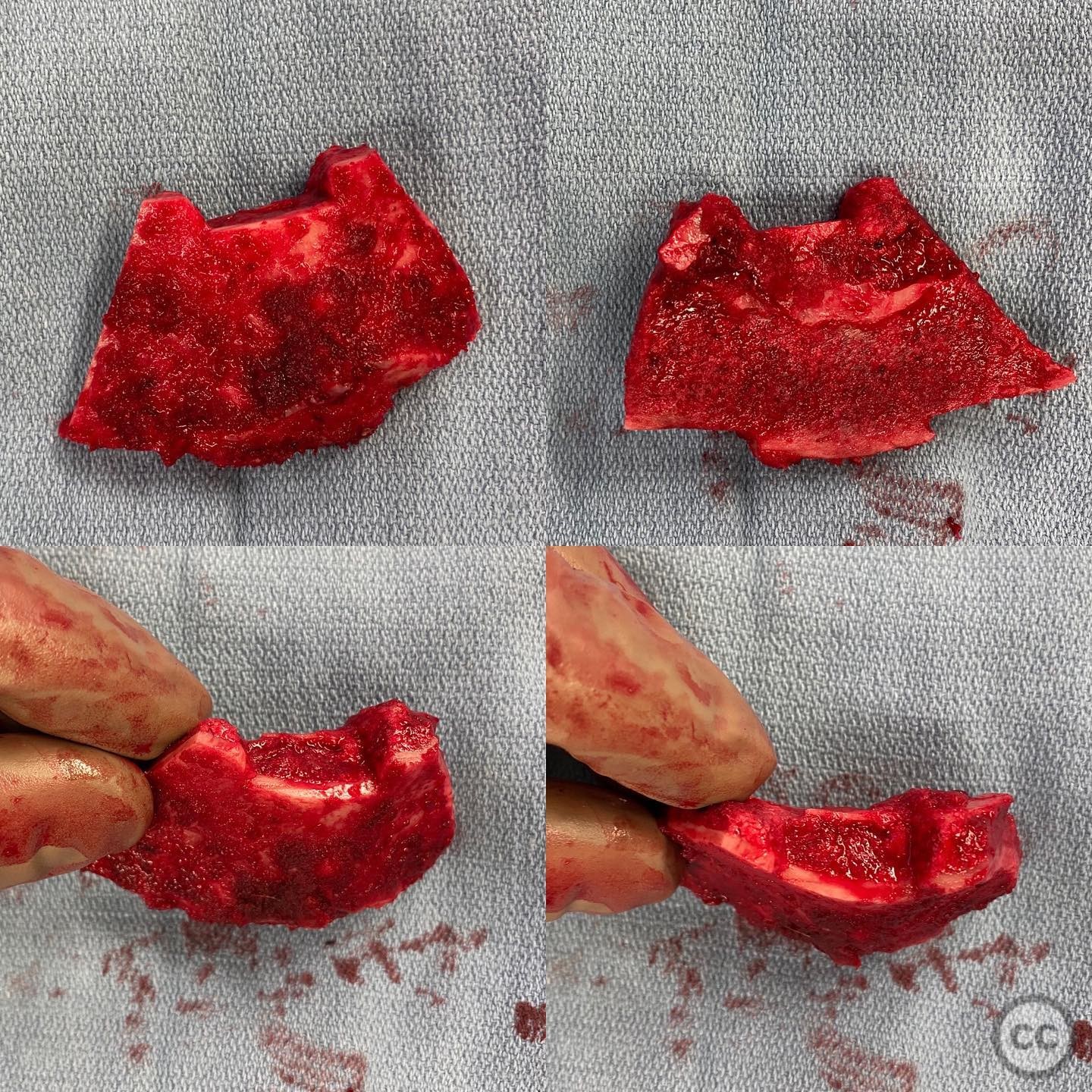
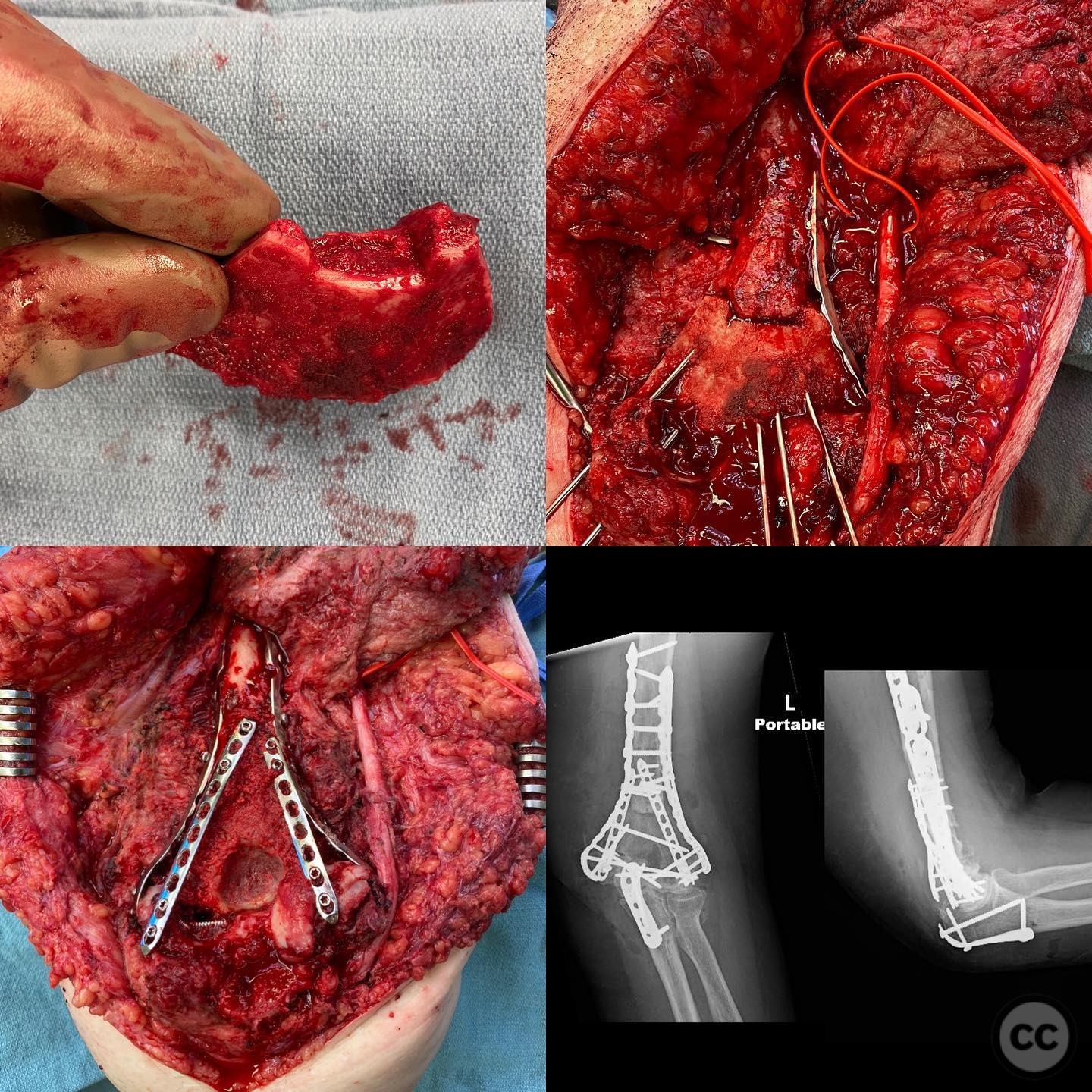
Planning remarks: The preoperative plan involved reconstruction of the distal humerus using a large autograft from the gluteal pillar to create a new metaphysis. The graft was to be step-cut on both ends for stability and trimmed to achieve correct coronal and sagittal alignment with symmetric compression. Additional fixation was planned to ensure stability.
Surgical Discussion
Patient positioning: The patient was positioned supine on the operating table with the affected arm placed on a radiolucent arm board to allow for optimal access and imaging.
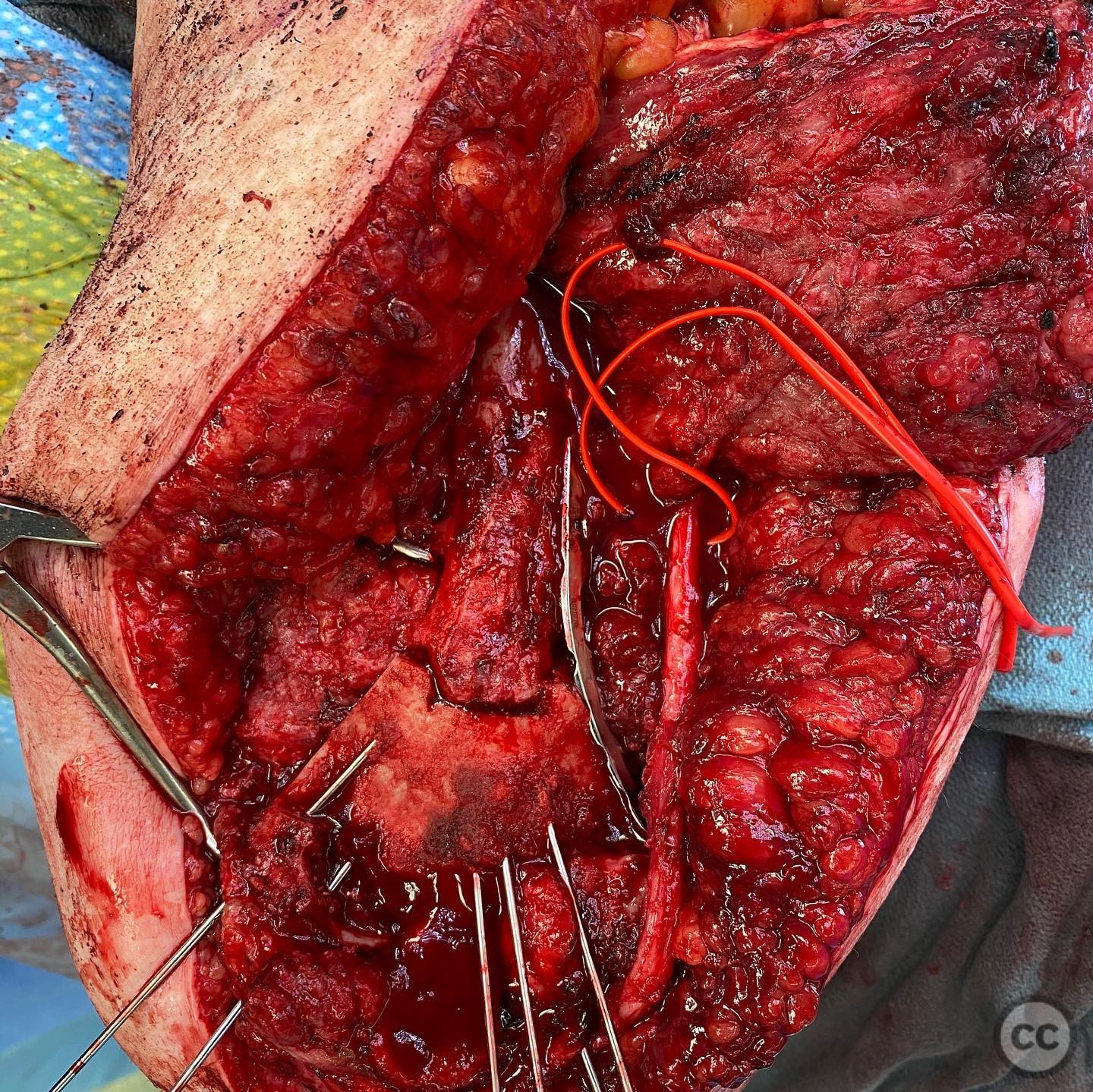
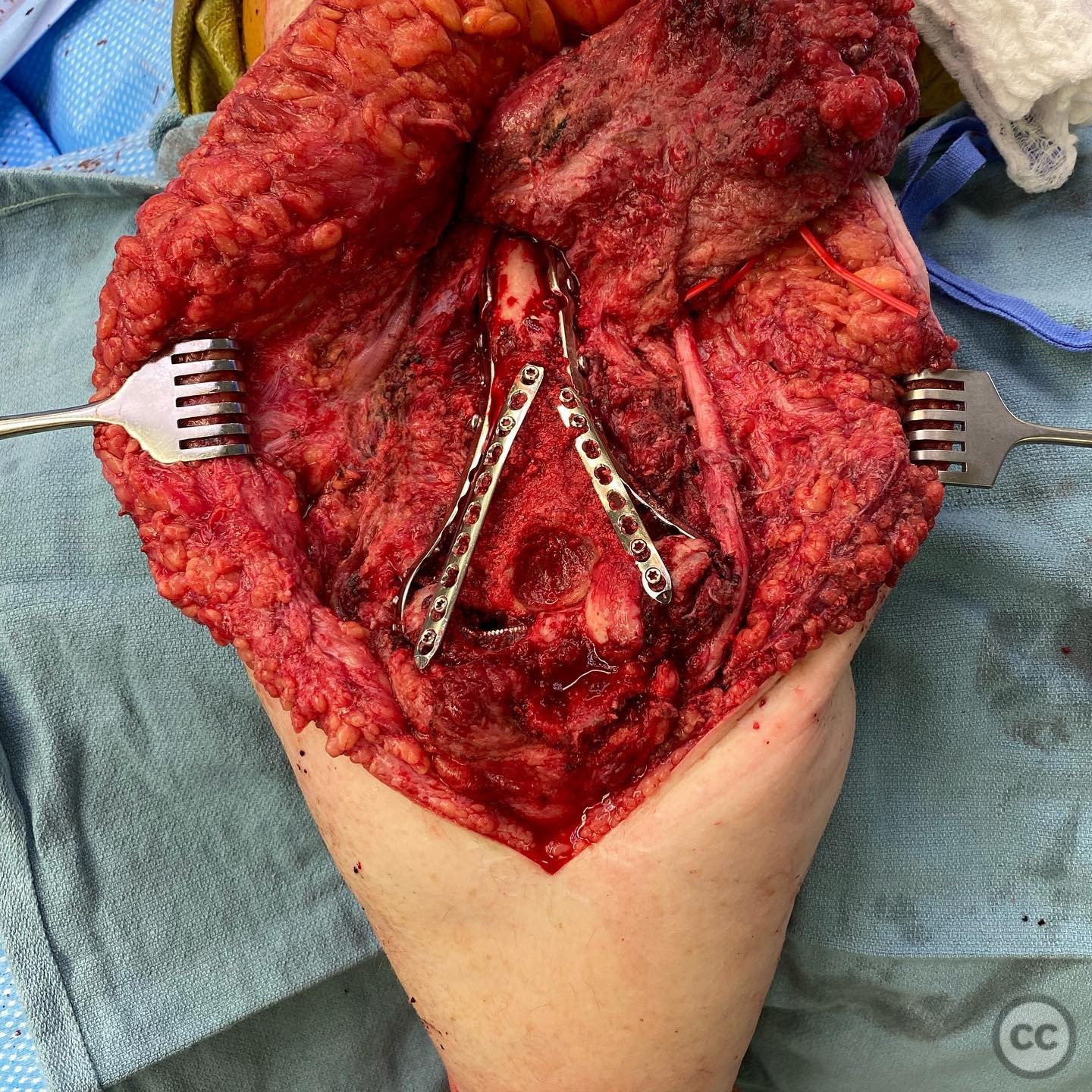
Anatomical surgical approach: A posterior approach to the distal humerus was utilized, involving an incision over the posterior aspect of the elbow. The triceps muscle was split longitudinally to expose the distal humerus. The nonunion site was debrided, and the segmental bone loss was addressed by placing the prepared gluteal pillar autograft into position. The graft was secured with step cuts for stability, and additional fixation was applied.
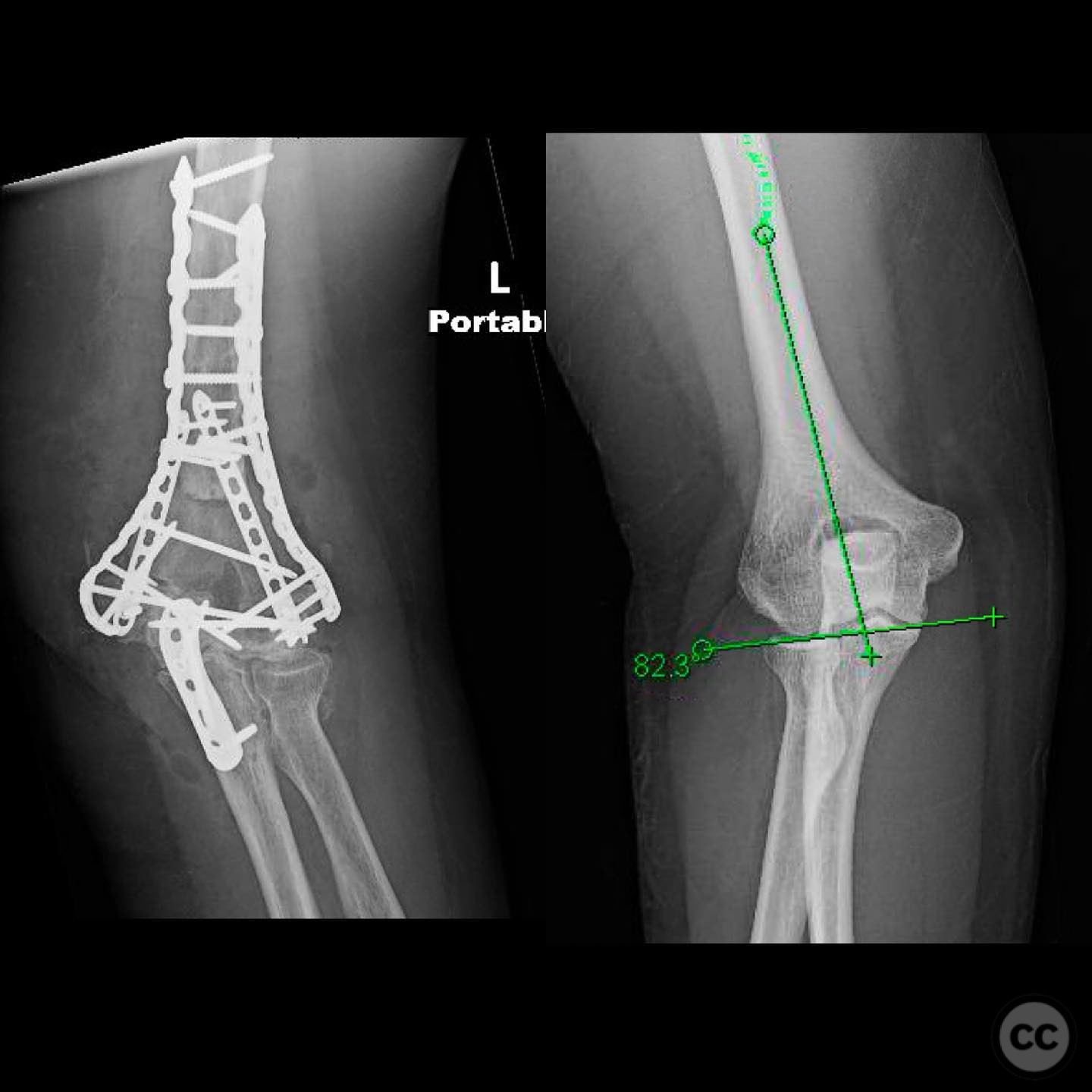
Operative remarks:The surgeon noted that the creation of a new olecranon fossa was necessary due to the segmental bone loss. Concerns were raised regarding potential elbow stiffness due to prolonged nonunion, which could increase load on the construct. Post-scar takedown, the patient achieved an unexpected range of motion from 10 to 120 degrees.
Postoperative protocol: Postoperative rehabilitation focused on maintaining elbow motion while protecting the reconstruction. Initial therapy aimed at gentle range of motion exercises within the achieved limits, progressing as tolerated.
Follow up: Not specified.
Orthopaedic implants used: Gluteal pillar autograft, additional fixation hardware (specific implants not detailed).
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 432 times
14 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Distal Humerus Nonunion with Segmental Bone Loss and Autograft Reconstruction.. Journal of Orthopaedic Surgery and Traumatology. Case Report 28967170 Published Online Jul 14 2025.