













Posterolateral Elbow Dislocation with Radial Head Fracture and Ligamentous Injury
Score and Comment on this Case
Clinical Details
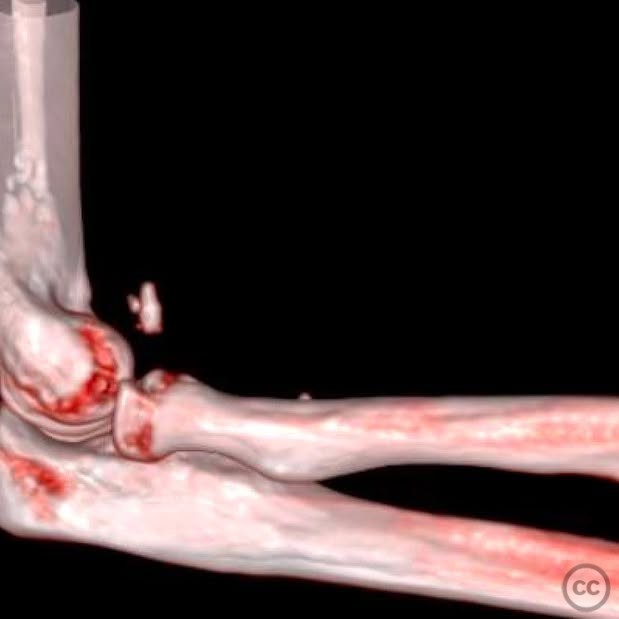
Clinical and radiological findings: A 24-year-old male sustained a fall while bouldering, landing on an outstretched arm. The patient presented with a closed injury to the elbow, without any neurological or vascular compromise. Radiological evaluation revealed a posterolateral elbow dislocation accompanied by a radial head/neck fracture, disruption of the lateral ulnar collateral ligament (LUCL) and annular ligament, anterior capsular and coronoid process involvement, and potential medial ulnar collateral ligament (MUCL) failure. The injury was classified as an AO/OTA 21-B2 fracture-dislocation.
Preoperative Plan
Planning remarks: The preoperative plan involved a lateral approach through the Kocher interval or via the traumatic rent. The surgical sequence included removal of loose osteochondral fragments, placement of heavy sutures in the anterior capsule with bone tunnels, fixation or replacement of the radial head, repair of the annular ligament, LUCL, and common extensor origin, followed by tying down the capsule and stability testing. A medial approach for MUCL repair was considered if instability persisted.
Surgical Discussion
Patient positioning: The patient was positioned supine with a varus creating bump placed under the elbow to facilitate access to anterior structures.
Anatomical surgical approach: A lateral approach was performed through the Kocher interval, involving an incision between the extensor carpi ulnaris and anconeus muscles. Subperiosteal dissection was carried out to expose the radial head and neck. The annular ligament and LUCL were repaired using suture anchors, and the common extensor origin was reattached to the lateral epicondyle.
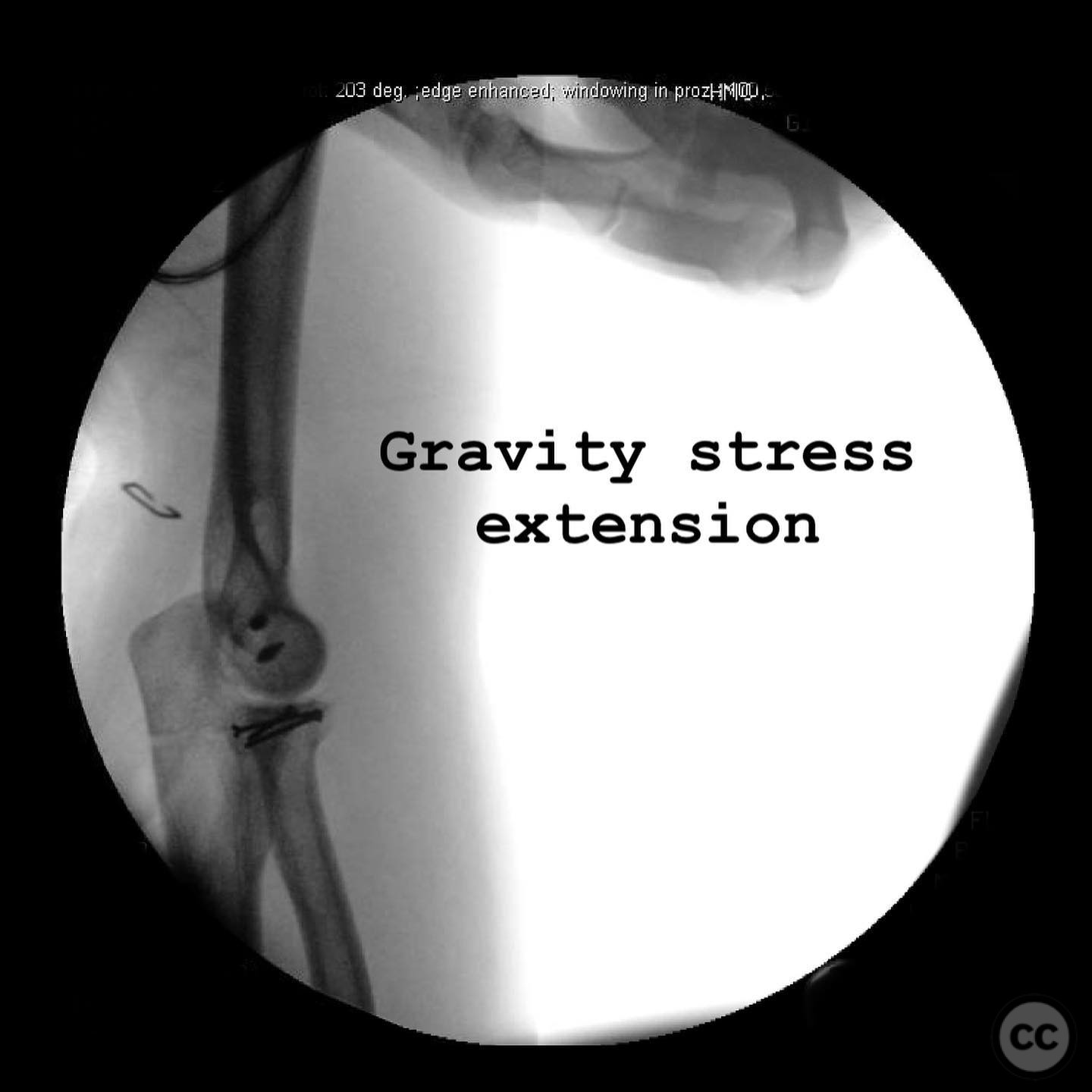
Operative remarks:The surgeon emphasized the importance of sequence in addressing this inherently unstable injury. The radial head was fixed or replaced based on fracture comminution. The annular ligament was repaired independently before addressing the LUCL with suture anchors at the isometric point. Stability assessment was conducted through various elbow positions to ensure concentric reduction of the radiocapitellar (RC) and ulnohumeral (UH) joints. Any instability detected between 30-90 degrees necessitated revision of the LUCL repair or additional stabilization measures.
Postoperative protocol: Postoperatively, the elbow was splinted in 90 degrees of flexion with full pronation. Immobilization duration was adjusted based on stability findings, with potential extension if instability was noted between 0-30 degrees.
Follow up: Not specified.
Orthopaedic implants used: Suture anchors for ligament repair, radial head prosthesis (if replacement was performed).
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 405 times
15 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Posterolateral Elbow Dislocation with Radial Head Fracture and Ligamentous Injury. Journal of Orthopaedic Surgery and Traumatology. Case Report 28703240 Published Online Jul 15 2025.