












Log Splitter Ankle Fracture Dislocation with Syndesmotic Injury.
Score and Comment on this Case
Clinical Details
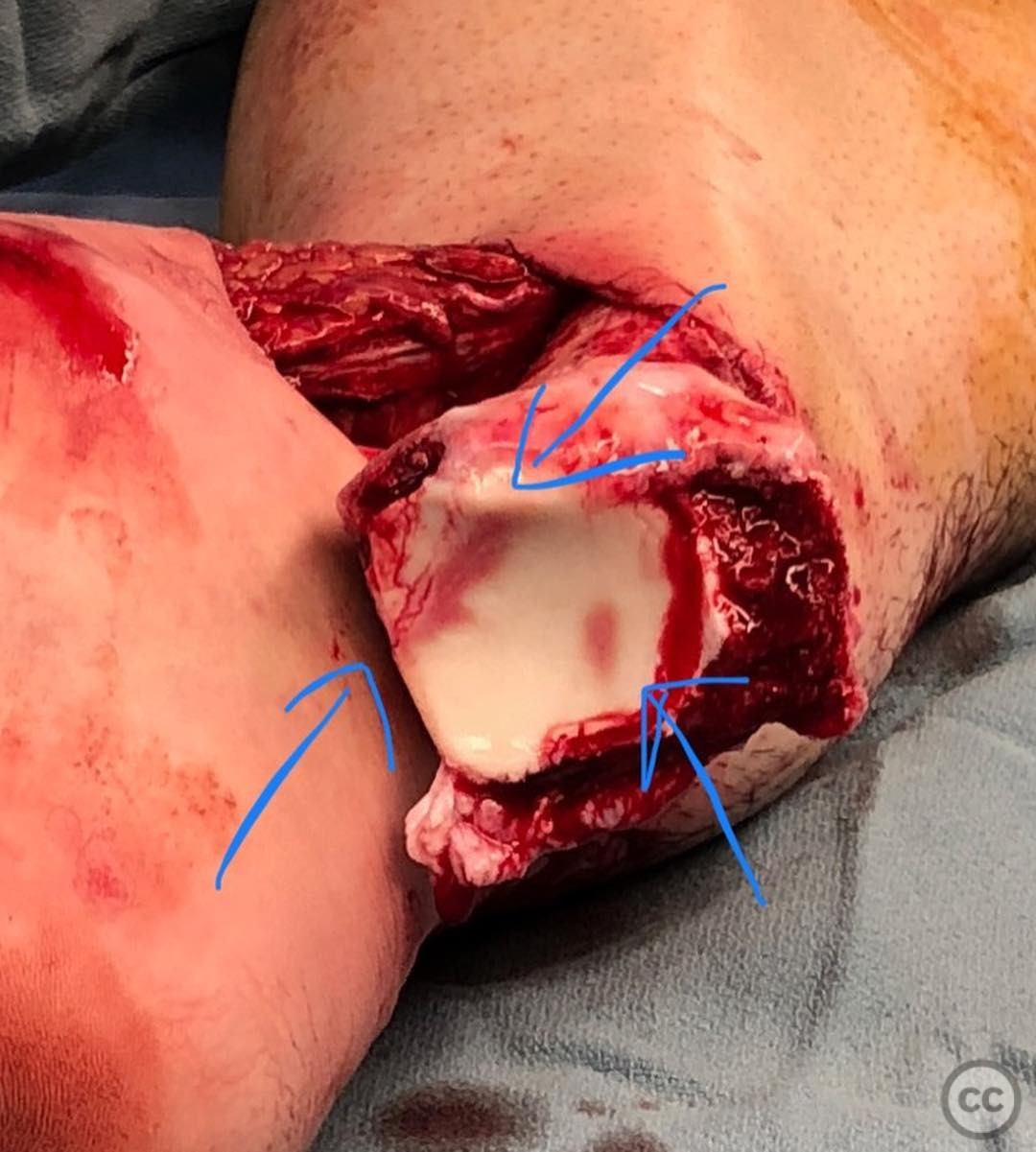
Clinical and radiological findings: A 31-year-old male sustained a fall from a height of 20 feet while bouldering at a gym, resulting in a "log splitter" ankle fracture dislocation. Initial clinical examination revealed significant swelling and deformity of the ankle joint. Radiographs indicated a complex fracture pattern, prompting the decision to obtain a post-reduction CT scan. The CT scan revealed an osteochondral fragment incarcerated in the incisura and a small Chaput fragment, with potential plafond involvement.
Preoperative Plan
Planning remarks: The preoperative plan included a thorough debridement of the joint, reduction and fixation of the Chaput fragment, and stabilization of the syndesmosis. A mini anterolateral approach was planned for addressing the Chaput fragment and syndesmosis. Supra-syndesmotic fibula fractures were to be plated using stacked 1/3 tubular plates.
Surgical Discussion
Patient positioning: The patient was positioned supine on the operating table with the affected limb elevated and supported to allow optimal access to the lateral and medial aspects of the ankle.
Anatomical surgical approach: A mini anterolateral approach was utilized, involving an incision over the anterolateral aspect of the ankle joint. Dissection proceeded through the subcutaneous tissue to expose the Chaput fragment and syndesmosis. Careful debridement was performed to remove the incarcerated osteochondral fragment from the incisura.
Operative remarks:The surgeon emphasized the importance of obtaining a CT scan for this fracture pattern to identify subtle findings that influence surgical planning. The presence of a Chaput fragment provided a bony equivalent for accurate syndesmotic reduction. Thorough debridement was essential to remove impediments to reduction, such as the osteochondral fragment. Stacked 1/3 tubular plates were preferred for fibular stabilization due to their stiffness and low profile.
Postoperative protocol: Postoperatively, the patient was placed in a splint with non-weight bearing status for 6 weeks. Progressive weight bearing was initiated thereafter, with physical therapy focusing on range of motion and strengthening exercises.
Follow up: Not specified.
Orthopaedic implants used: Stacked 1/3 tubular plates, 3.0mm screws for medial malleolus fixation.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 516 times
25 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Log Splitter Ankle Fracture Dislocation with Syndesmotic Injury.. Journal of Orthopaedic Surgery and Traumatology. Case Report 28648268 Published Online Jul 25 2025.