















Complex Floating Knee with Vascular Compromise and Proximal Tibiofibular Joint Dislocation
Score and Comment on this Case
Clinical Details
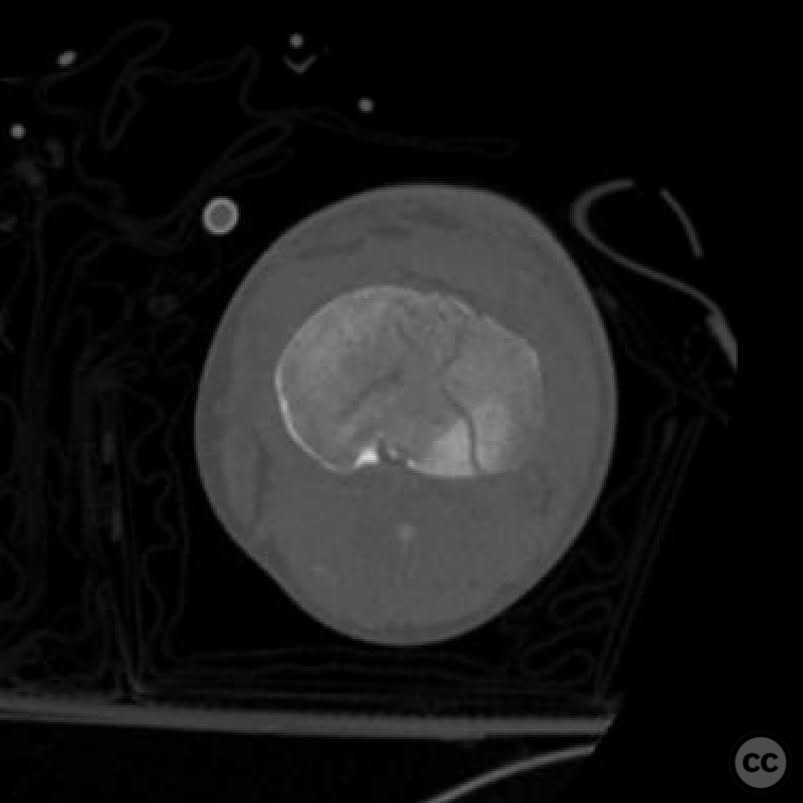
Clinical and radiological findings: A 39-year-old male involved in a motorcycle accident presented with a polytrauma including a floating knee injury. The patient had no palpable pulses, and a CTA revealed no flow at the trifurcation with reconstitution through the peroneal artery at the ankle level. The foot appeared perfused. The femur fracture was 3cm open anteromedially, while the tibia fracture was closed. The patient was intubated and sedated, precluding a neurological examination. No major head, chest, or abdominal injuries were noted.
Preoperative Plan
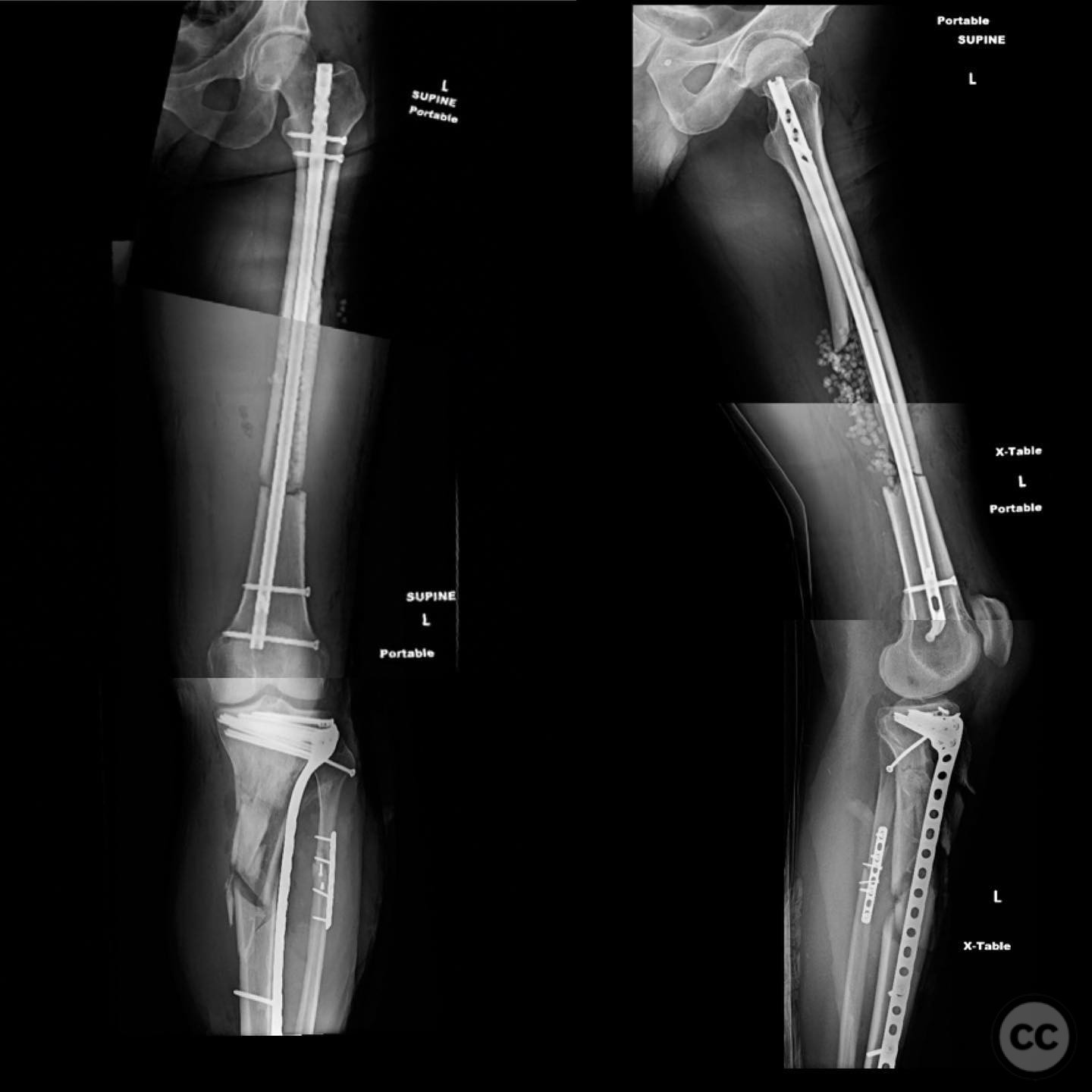
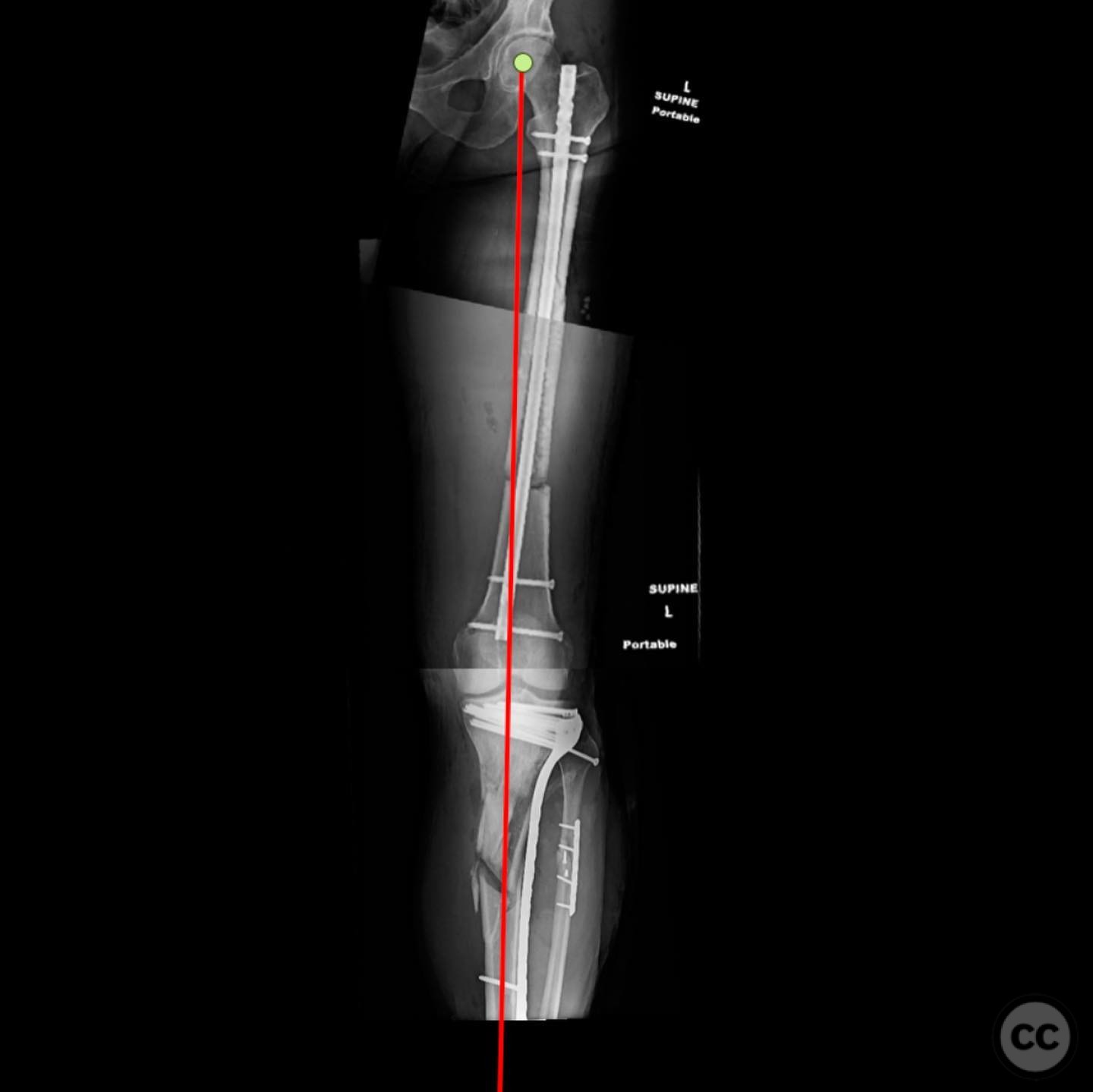
Planning remarks: The preoperative plan involved addressing the open femur fracture first, using an extensile lateral approach for debridement and irrigation, followed by intramedullary nailing. For the tibia, the plan included reduction and fixation of the fibula, articular surface of the tibial plateau, proximal tibiofibular joint (PTFJ), and finally bridging plate fixation of the tibia.
Surgical Discussion
Patient positioning: The patient was positioned supine on the operating table to facilitate access to both the femur and tibia.
Anatomical surgical approach: An extensile lateral approach was utilized for the femur, allowing for thorough debridement and irrigation of the open fracture site. For the tibia, a medial approach was employed, using a distractor to restore length after fibular fixation. This approach also facilitated access for vascular repair and fasciotomies.
Operative remarks:During femoral fixation, devitalized bone segments were used as templates before being discarded post-nailing. The anterior intercalary fragment retained good muscle attachment, suggesting potential for healing, though bone grafting may be necessary. Intraoperatively, upon achieving tibial length restoration, a vascular injury occurred, managed with digital pressure and a sterile tourniquet until vascular surgery performed a sidewall repair. Fasciotomies were completed prior to final fixation.
Postoperative protocol: Postoperatively, the patient received a split-thickness skin graft (STSG) for fasciotomy wound coverage. The leg remained well perfused.
Follow up: Not specified
Orthopaedic implants used: Intramedullary nail for femur fixation, bridging plate for tibial fixation, distractor for length restoration, sterile tourniquet for vascular control.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 299 times
14 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Complex Floating Knee with Vascular Compromise and Proximal Tibiofibular Joint Dislocation. Journal of Orthopaedic Surgery and Traumatology. Case Report 28244887 Published Online Jul 14 2025.