


Monteggia Fracture-Dislocation with Posterior Radiocapitellar Dislocation
Score and Comment on this Case
Clinical Details
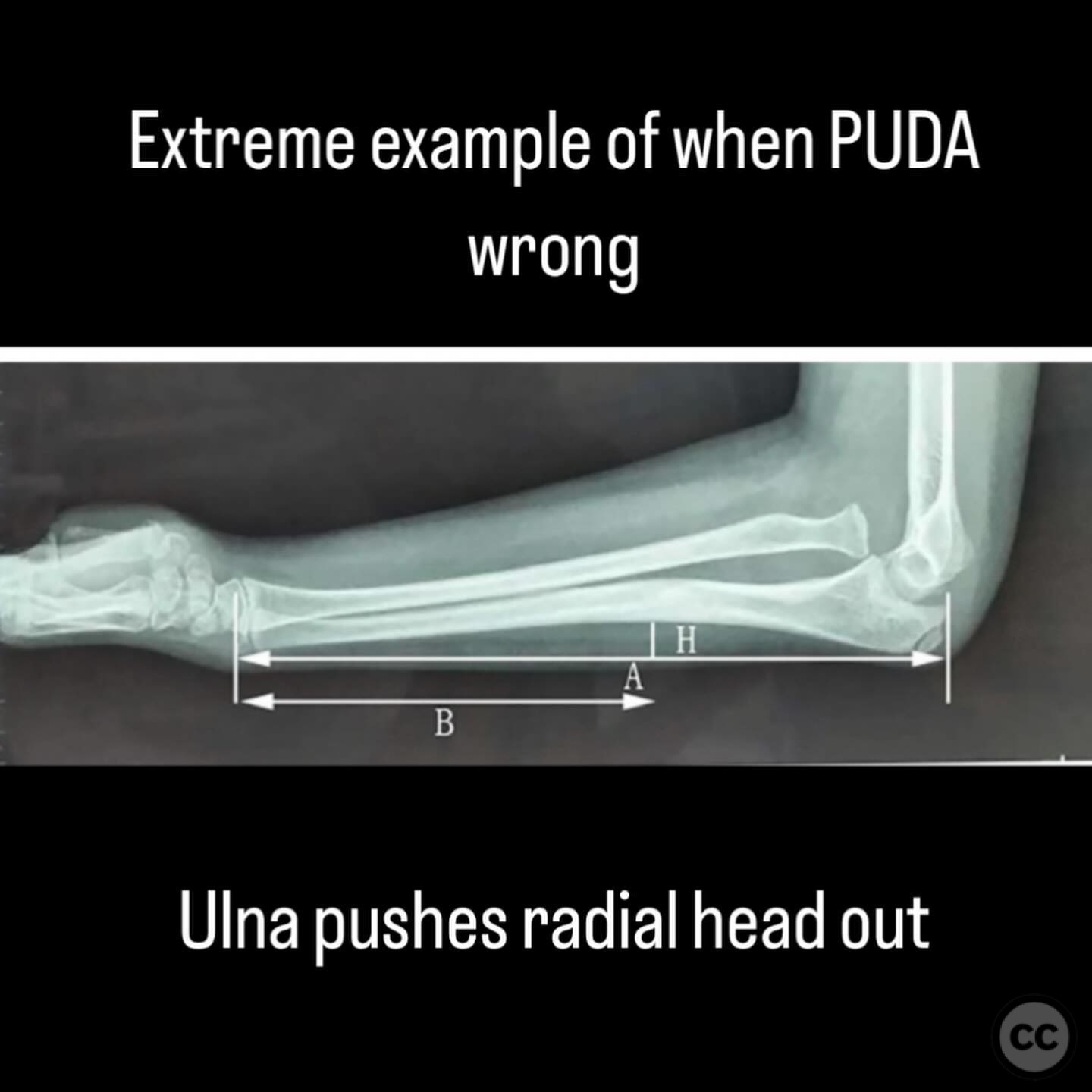
Clinical and radiological findings: A 43-year-old male sustained a fall from a cliff while snowmobiling, resulting in a Monteggia fracture-dislocation. The injury is characterized by a fracture of the proximal ulna with an associated posterior dislocation of the radiocapitellar joint. Initial clinical examination revealed significant swelling of the forearm, raising concerns for potential compartment syndrome. Radiographic evaluation confirmed the fracture-dislocation pattern, and the complexity of the proximal ulnar morphology was noted, which is critical for achieving proper reduction and stability of the radiocapitellar joint.
Preoperative Plan
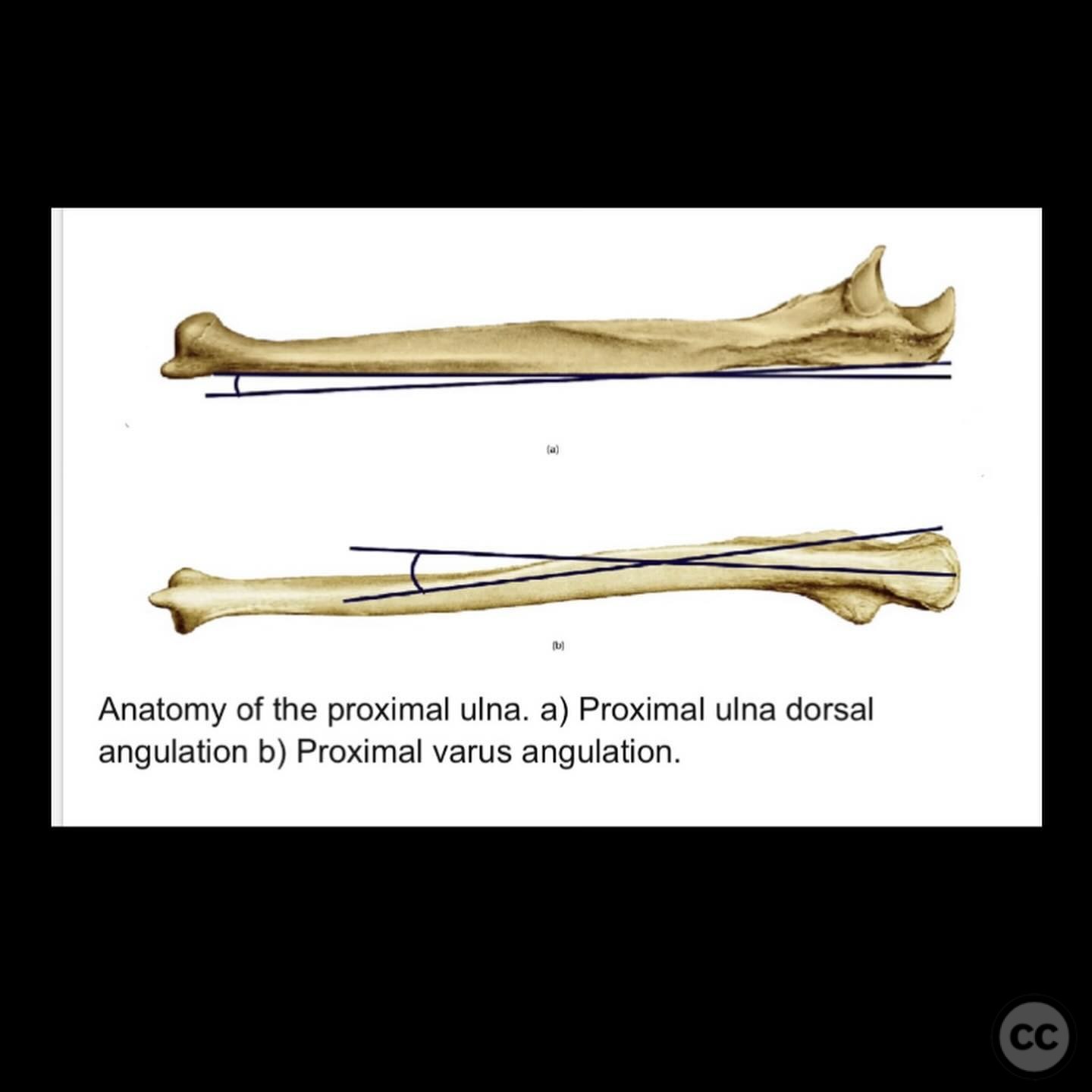
Planning remarks: The preoperative plan involved a posterior approach to the proximal ulna to allow for direct visualization and reduction of the fracture. Restoration of the proximal ulnar dorsal angulation (PUDA) and natural varus bow was emphasized to ensure proper alignment and function of the radiocapitellar and proximal radioulnar joints. Attention was given to potential complications such as buttonholed capsule or flipped annular ligament.
Surgical Discussion
Patient positioning: The patient was positioned supine with the affected arm placed on a radiolucent hand table to facilitate intraoperative imaging and manipulation.
Anatomical surgical approach: A posterior longitudinal incision was made along the proximal ulna. Subperiosteal dissection was performed to expose the fracture site. Careful attention was given to preserving soft tissue attachments and identifying key anatomical landmarks to guide accurate reduction.
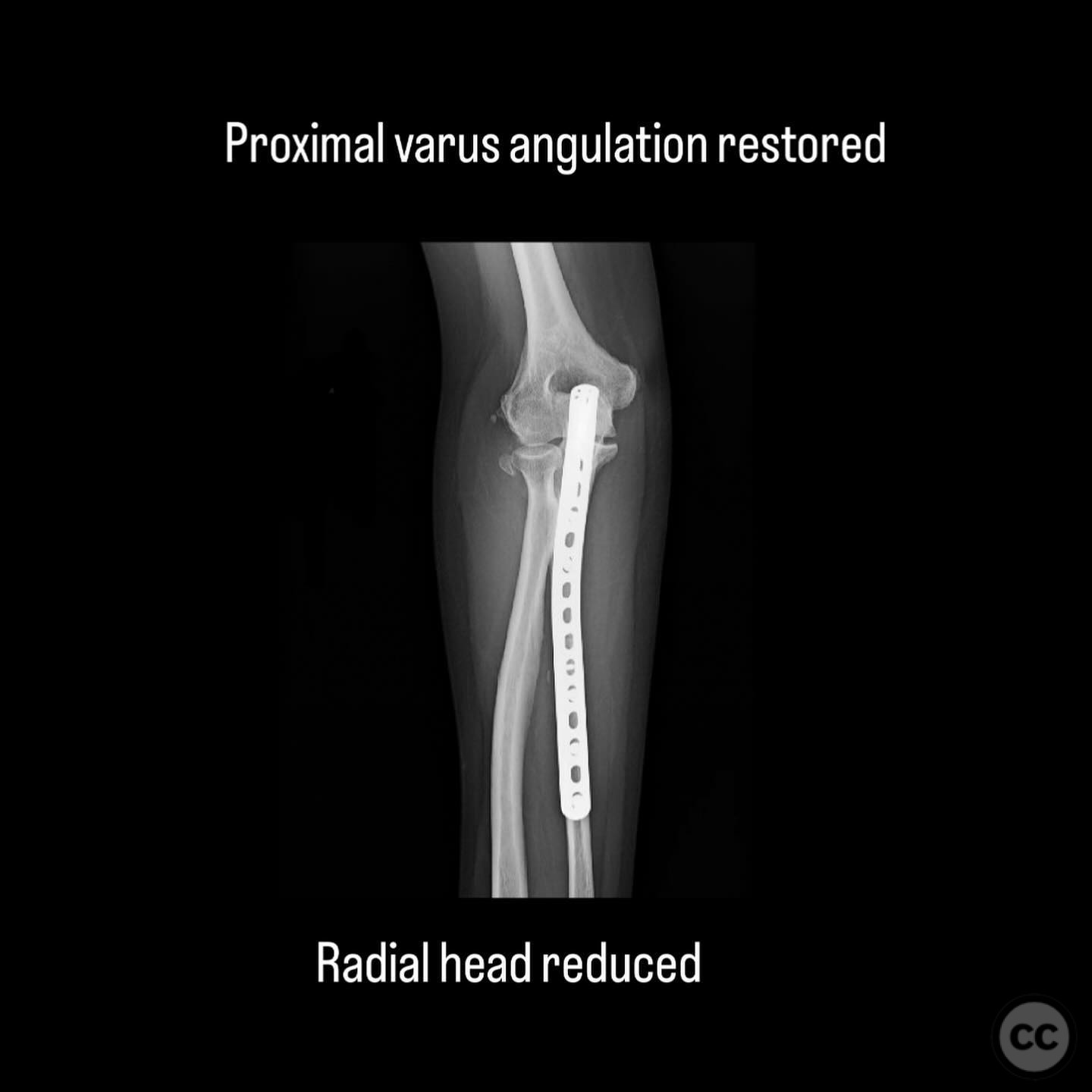
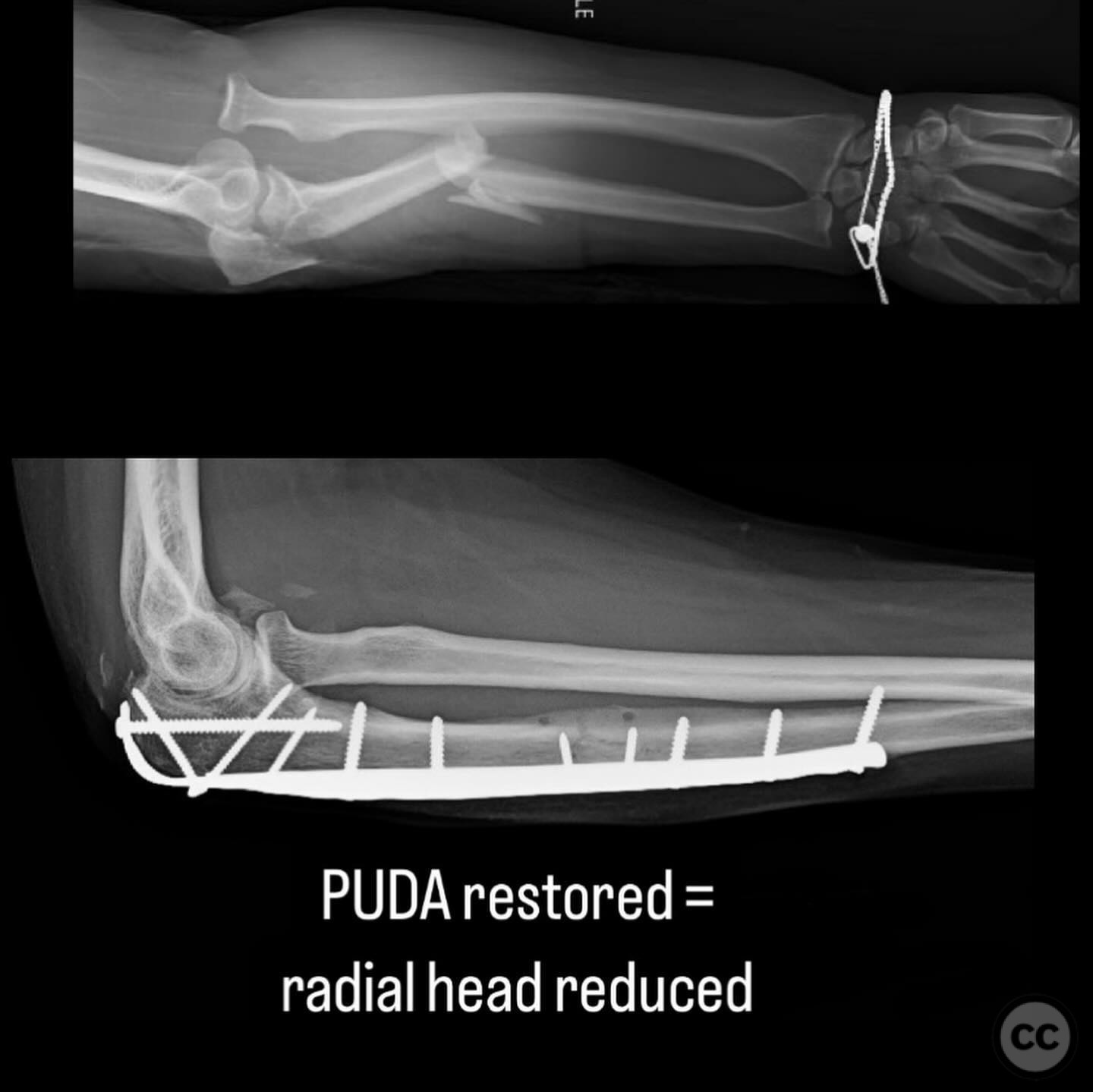
Operative remarks:The surgeon noted the importance of restoring the PUDA and natural varus bow of the ulna to prevent malalignment of the radiocapitellar joint. The complexity of the proximal ulnar architecture required meticulous attention to detail during reduction. Despite achieving anatomical reduction, vigilance was maintained for potential soft tissue interposition, such as a buttonholed capsule or flipped annular ligament, which could impede joint stability.
Postoperative protocol: Postoperatively, the patient was placed in a splint with the elbow in 90 degrees of flexion and forearm in neutral rotation. Early passive range of motion exercises were initiated within the first week, with progression to active-assisted exercises by week 3. Weight-bearing restrictions were maintained until radiographic evidence of healing was observed.
Follow up: Not specified.
Orthopaedic implants used: Locking compression plate (LCP) for proximal ulna fixation.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 248 times
10 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Monteggia Fracture-Dislocation with Posterior Radiocapitellar Dislocation. Journal of Orthopaedic Surgery and Traumatology. Case Report 28098395 Published Online Jul 10 2025.