





 bone loss wrap up ☠️_._._._If just joining_ please check back a few posts for the injury films a(.jpg)
 bone loss wrap up ☠️_._._._If just joining_ please check back a few posts for the injury films _2.jpg)
 bone loss wrap up ☠️_._._._If just joining_ please check back a few posts for the injury films _1.jpg)
 bone loss wrap up ☠️_._._._If just joining_ please check back a few posts for the injury films _3.jpg)
 bone loss wrap up ☠️_._._._If just joining_ please check back a few posts for the injury films _4.jpg)
 bone loss wrap up ☠️_._._._If just joining_ please check back a few posts for the injury films _5.jpg)
 bone loss wrap up ☠️_._._._If just joining_ please check back a few posts for the injury films _6.jpg)
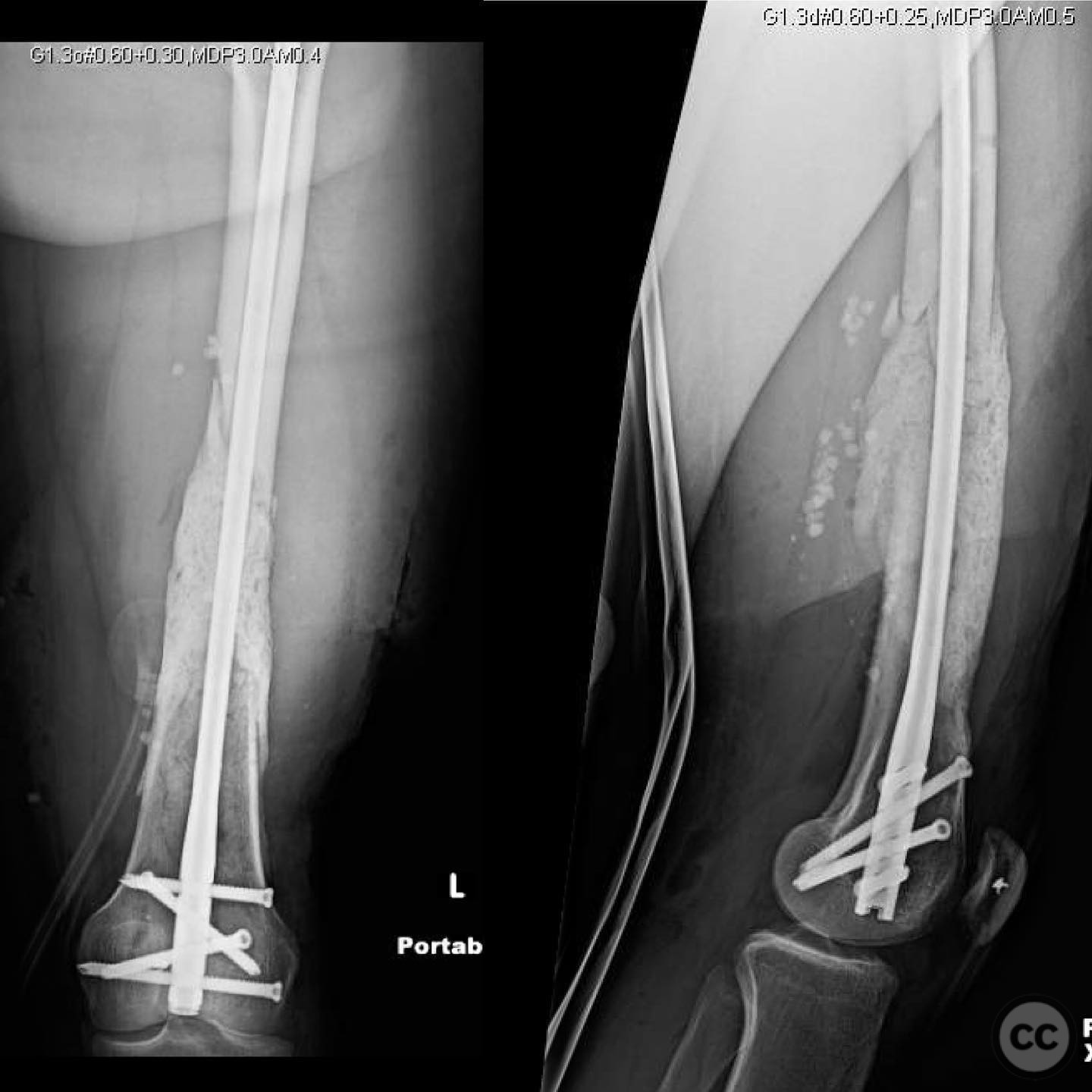
Masquelet Technique in Management of 3a Open Diaphyseal Femur Fracture with Segmental Bone Loss
Score and Comment on this Case
Clinical Details
Clinical and radiological findings: A young male patient presented with a 3a open diaphyseal femur fracture accompanied by a significant 12cm segmental bone loss. The initial injury was heavily contaminated. The patient underwent staged treatment involving external fixation, intramedullary nailing, and cement spacer placement as part of the Masquelet technique. There was no history of infection, and cultures at the time of bone grafting were negative. Laboratory tests including ESR, CRP, and WBC were within normal limits, and nonunion labs were normal.
Preoperative Plan
Planning remarks: The preoperative plan involved the Masquelet technique, which included the initial placement of a cement spacer to induce membrane formation, followed by autologous bone grafting to address the segmental defect. The expectation was that multiple operations might be necessary to achieve complete bone healing.
Surgical Discussion
Patient positioning: Supine positioning on a radiolucent table to facilitate intraoperative imaging and access to the femoral diaphysis.
Anatomical surgical approach: A lateral approach to the femur was utilized, involving an incision over the lateral aspect of the thigh. Dissection proceeded through the fascia lata to expose the femoral shaft. Care was taken to preserve soft tissue integrity around the fracture site.
Operative remarks:The initial bone grafting significantly reduced the segmental defect from 12cm to a smaller size. The Masquelet technique was not considered a failure as it often requires multiple grafting procedures for large defects. The surgical team emphasized the importance of patient understanding regarding the potential need for additional operations. Alternative strategies such as corticotomy and transport using external frames or nail transport were considered but required high patient compliance.
Postoperative protocol: Postoperative rehabilitation included limited weight-bearing with gradual progression as tolerated. Regular follow-up was essential to monitor bone healing and integration of the graft.
Follow up: Not specified.
Orthopaedic implants used: External fixator, intramedullary nail, cement spacer, autologous bone graft.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 350 times
15 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Masquelet Technique in Management of 3a Open Diaphyseal Femur Fracture with Segmental Bone Loss. Journal of Orthopaedic Surgery and Traumatology. Case Report 27151235 Published Online Jul 15 2025.