





Posterior Wall Acetabular Fracture-Dislocation in a Young Athlete: Open Reduction and Internal Fixation with Spring-Hook and Recon Plate
Score and Comment on this Case
Clinical Details
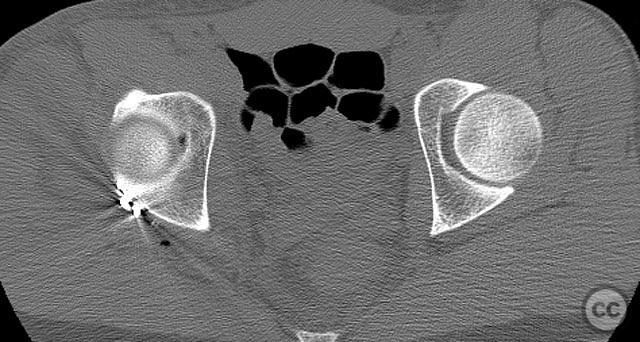
Clinical and radiological findings: A 20-year-old male collegiate basketball player sustained a displaced right posterior wall (PW) acetabular fracture-dislocation during practice. Initial AP pelvic radiograph demonstrated a reduced femoral head with a displaced posterior wall fragment. Axial CT imaging revealed a large, peripherally located PW fragment with significant displacement, impaction into the abductor muscle mass, and no intra-articular comminution. Obturator oblique radiographs and intraoperative fluoroscopy under anesthesia demonstrated mechanical obstruction to passive abduction at 10–20 degrees due to the relationship between the displaced PW fragment and the greater trochanter.
Preoperative Plan
Planning remarks: The preoperative plan was for open reduction and internal fixation of the posterior wall fragment via a Kocher-Langenbeck (KL) approach. The technical plan included careful dissection to avoid further devascularization of the fragment, direct fragment mobilization, reduction, and fixation using a spring-hook implant for fragment capture and a supporting reconstruction plate placed medial to the hook tines.
Surgical Discussion
Patient positioning: The patient was positioned in the lateral decubitus position with the affected side up, allowing optimal access to the posterior column and wall of the acetabulum.
Anatomical surgical approach: A standard Kocher-Langenbeck approach was utilized. A longitudinal incision was made centered over the greater trochanter, extending proximally along the posterior iliac crest and distally along the femoral shaft. The fascia lata was incised, and the gluteus maximus was split in line with its fibers. The short external rotators (piriformis, obturator internus, gemelli) were identified, tagged, and released from their femoral insertions to expose the posterior aspect of the acetabulum. The sciatic nerve was identified and protected throughout. The posterior wall fragment, found impaled within the abductor muscle mass, was mobilized with minimal additional soft tissue stripping. Open reduction was achieved, and fixation was performed using a spring-hook implant applied directly to the bony fragment (avoiding labral capture), with a reconstruction plate contoured and placed just medial to the hook tines for additional support. All screws were placed extra-articularly.
Operative remarks:Intraoperatively, the posterior wall fragment was found firmly embedded within the abductor musculature, necessitating careful disimpaction and minimal periosteal stripping to preserve vascularity. The spring-hook device provided secure capture of the peripheral fragment without involving the labrum. Placement of the reconstruction plate medial to the hook tines provided buttress support to prevent secondary displacement. Fluoroscopic imaging confirmed anatomic reduction and extra-articular screw placement. Postoperative CT demonstrated satisfactory reduction and implant positioning.
Postoperative protocol: Early passive range of motion exercises were initiated postoperatively, avoiding hip flexion beyond 90 degrees and abduction beyond 20 degrees for six weeks. Toe-touch weight bearing was maintained for six weeks, progressing to partial weight bearing at eight weeks, and full weight bearing as tolerated by twelve weeks. Return to athletic activity was permitted at four months post-injury following clinical and radiographic confirmation of healing.
Follow up: At one year post-injury, radiographs demonstrated maintained reduction and implant integrity. The patient returned to competitive basketball four months after surgery without restriction.
Orthopaedic implants used: Spring-hook acetabular fixation device; 3.5 mm reconstruction plate; cortical screws (extra-articular).
Search for Related Literature


Industry Sponsership
contact us for advertising opportunities
Article viewed 321 times
11 Sep 2025
Add to Bookmarks
Full Citation
Cite this article:
Routt, ML. (2025). Posterior Wall Acetabular Fracture-Dislocation in a Young Athlete: Open Reduction and Internal Fixation with Spring-Hook and Recon Plate. Journal of Orthopaedic Surgery and Traumatology. Case Report 26809036 Published Online Sep 11 2025.