

.jpg)


Early Percutaneous Stabilization of Complex Pelvic and Proximal Femoral Fractures in a Polytraumatized Elderly Patient
Score and Comment on this Case
Clinical Details
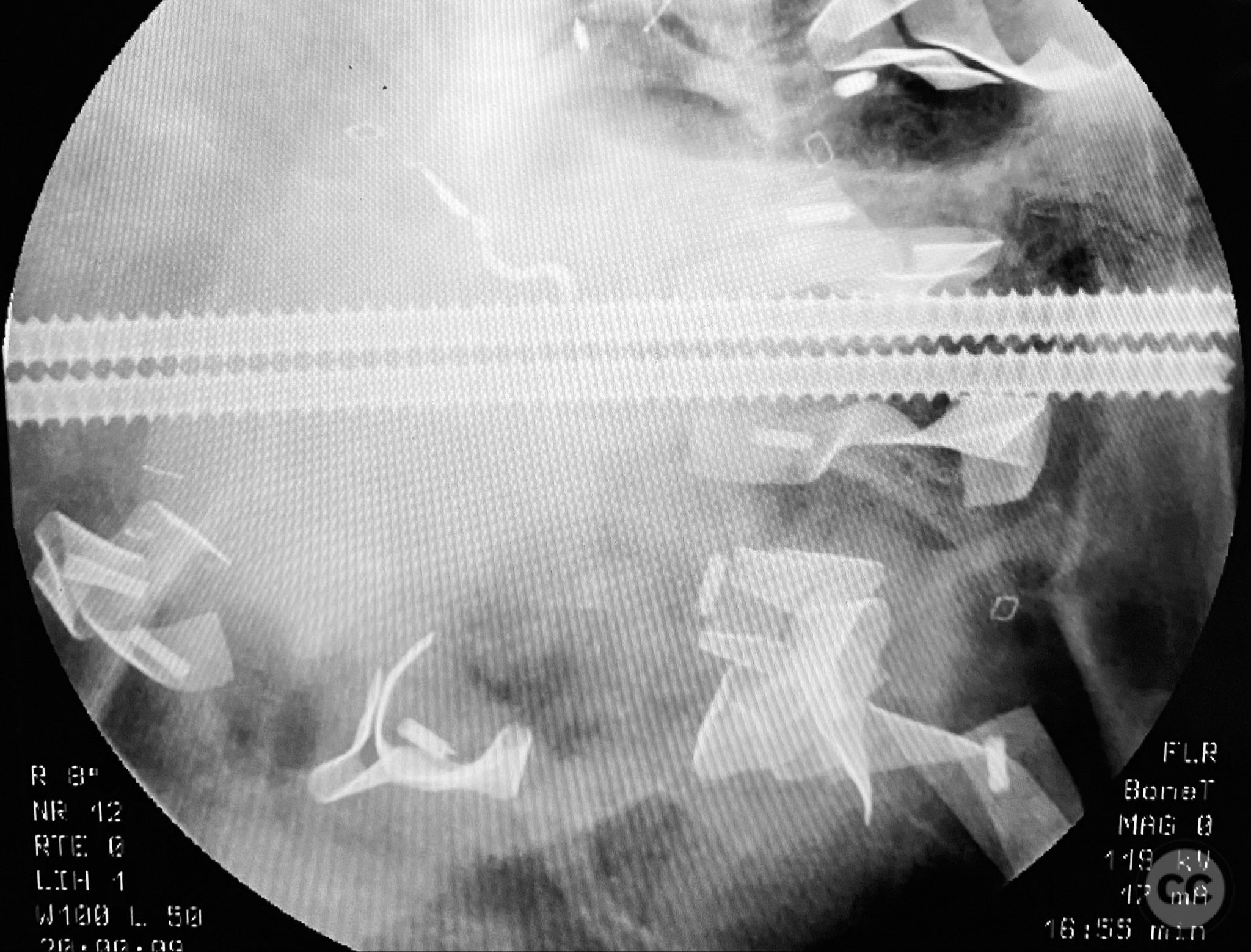
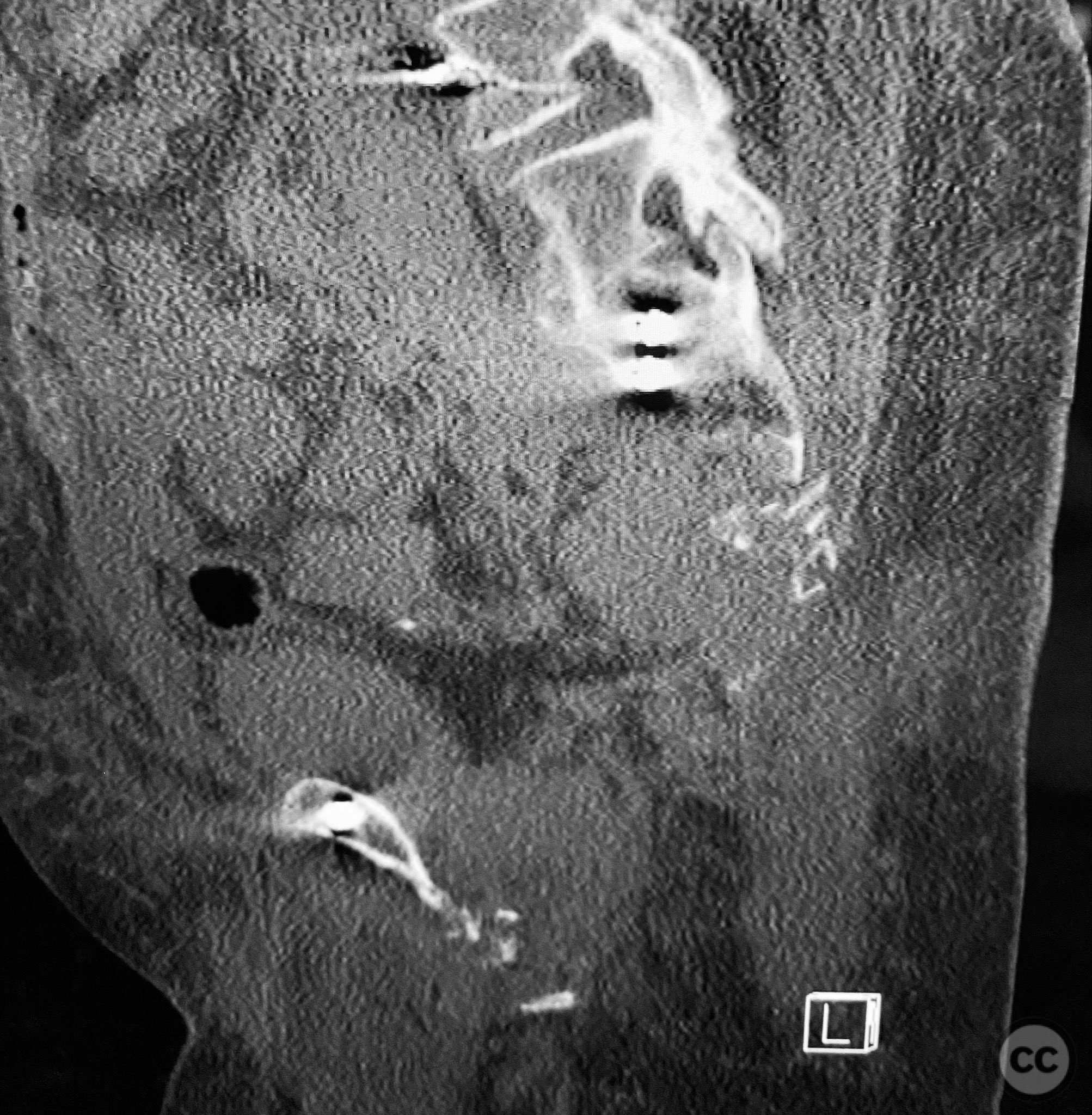
Clinical and radiological findings: An elderly patient sustained multiple traumatic injuries, including complex unstable pelvic ring disruption (AO/OTA 61-C, likely C1 or C2 based on instability and comminution), comminuted proximal femoral fracture (AO/OTA 31-A3 or 31-B, depending on trochanteric or neck involvement), and significant abdominal trauma necessitating intra-abdominal packing. Initial clinical evaluation revealed hemodynamic instability and poor bone quality consistent with advanced age. Distal femoral traction was applied for provisional reduction. Radiological assessment was limited by osteopenia, fracture comminution, and the presence of abdominal packing materials.
Preoperative Plan
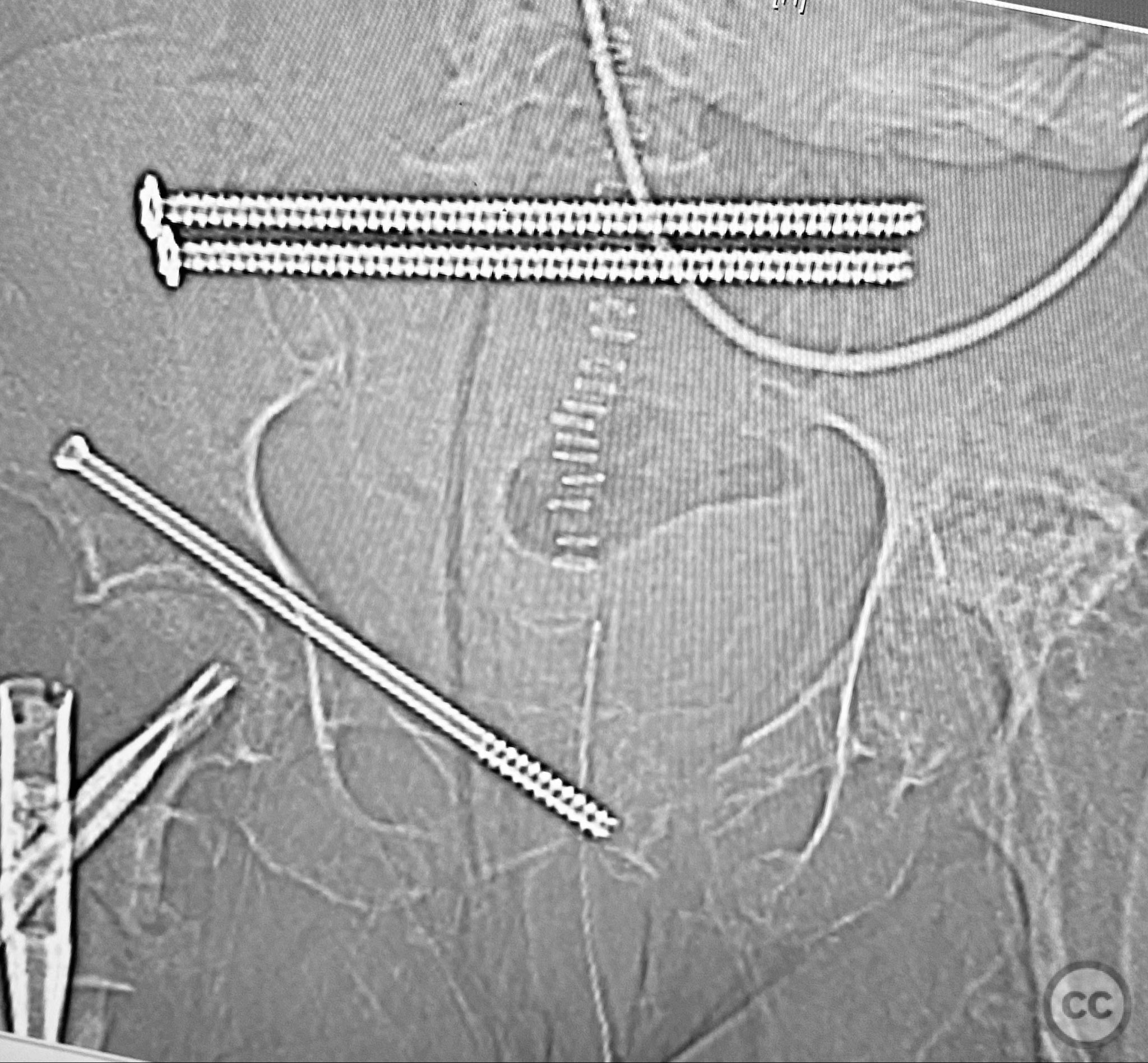
Planning remarks: The preoperative plan included early closed reduction maneuvers under fluoroscopic guidance, percutaneous stabilization of the pelvic ring with cannulated screws, and intramedullary nailing of the proximal femur. The anatomical approach for pelvic fixation was percutaneous iliosacral screw placement; for the femur, a standard antegrade intramedullary nailing technique was planned.
Surgical Discussion
Patient positioning: The patient was positioned supine on a radiolucent operating table to facilitate access to the pelvis and proximal femur, with the affected limb in traction via a distal femoral pin.
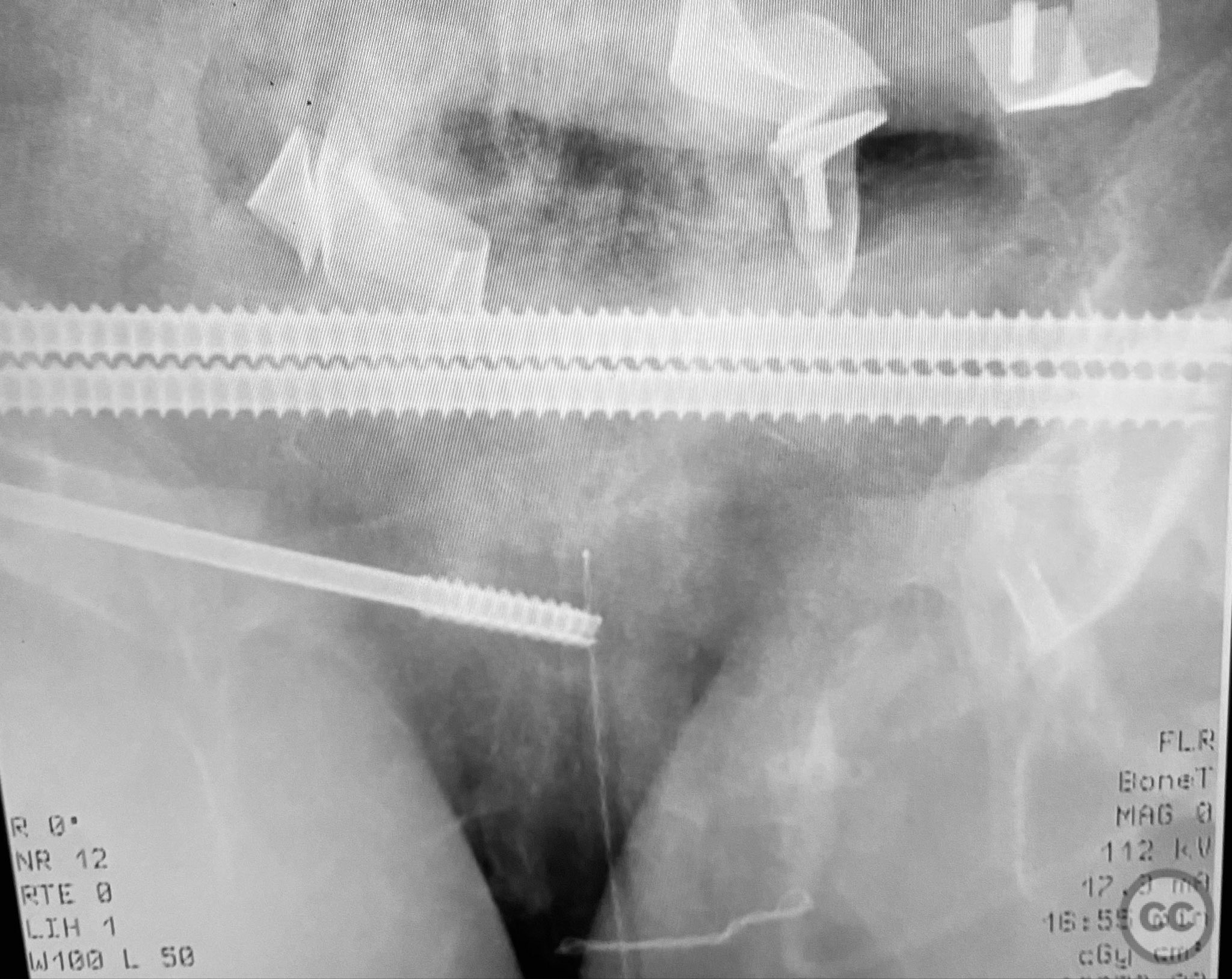
Anatomical surgical approach: Percutaneous iliosacral screw fixation was performed through small lateral gluteal incisions, with blunt dissection to the outer table of the os ilium. Under fluoroscopic guidance, guidewires were advanced across the sacroiliac joint into the S1 body, followed by cannulated screw insertion. For the proximal femur, a longitudinal incision was made proximal to the greater trochanter, splitting the fascia lata and gluteus medius fibers to access the piriformis fossa. A guidewire was inserted into the medullary canal, followed by sequential reaming and insertion of an intramedullary nail.
Operative remarks:Intraoperative imaging was challenging due to osteopenic bone, fracture comminution, and interference from abdominal packing. Accurate identification of safe osseous corridors for iliosacral screw placement required multiple fluoroscopic projections and careful attention to pelvic landmarks. Bone quality necessitated cautious screw advancement to avoid iatrogenic cortical breach. After pelvic fixation, intramedullary nailing of the proximal femur proceeded without complication. Abdominal packing was removed and laparotomy wound closed after skeletal stabilization. Early mechanical stabilization of both pelvic and femoral injuries was prioritized to optimize survivability in this multiply injured elderly patient.
Postoperative protocol: Postoperatively, early mobilization with protected weight bearing as tolerated was initiated, with physiotherapy focusing on respiratory function and prevention of decubitus complications. Deep vein thrombosis prophylaxis and close monitoring for systemic complications were instituted.
Follow up: Not specified
Orthopaedic implants used: Cannulated iliosacral screws, antegrade intramedullary femoral nail
Search for Related Literature


Industry Sponsership
contact us for advertising opportunities
Article viewed 699 times
12 Sep 2025
Add to Bookmarks
Full Citation
Cite this article:
Routt, ML. (2025). Early Percutaneous Stabilization of Complex Pelvic and Proximal Femoral Fractures in a Polytraumatized Elderly Patient. Journal of Orthopaedic Surgery and Traumatology. Case Report 26478220 Published Online Sep 12 2025.