









Supramalleolar Osteotomy for Distal Tibia and Fibula Malunion in a Diabetic Patient with Peripheral Neuropathy
Score and Comment on this Case
Clinical Details
Clinical and radiological findings: A 52-year-old male with type 1 diabetes and dense peripheral neuropathy presented with foot swelling persisting for several weeks. The patient is highly compliant with diabetes management, maintaining an A1C of 6.9. Vascular studies indicated excellent peripheral inflow and outflow, with the medial skin in good condition and lateral skin noted to be very supple. Radiological evaluation revealed a malunion of the distal tibia and fibula, secondary to a low-energy pilon fracture of unknown chronicity.
Preoperative Plan
Planning remarks: The preoperative plan involved an anterolateral approach to address the distal tibial malunion. Given the uncertainty regarding the healing status of the tibia, the surgical strategy included either reduction and fixation or performing an osteotomy followed by fixation. A supramalleolar opening wedge osteotomy at the Cora was planned to restore native anatomy, with subsequent adjustment of the fibula to match the corrected tibial alignment.
Surgical Discussion
Patient positioning: The patient was positioned supine on the operating table, with the affected limb prepared for lateral distraction.
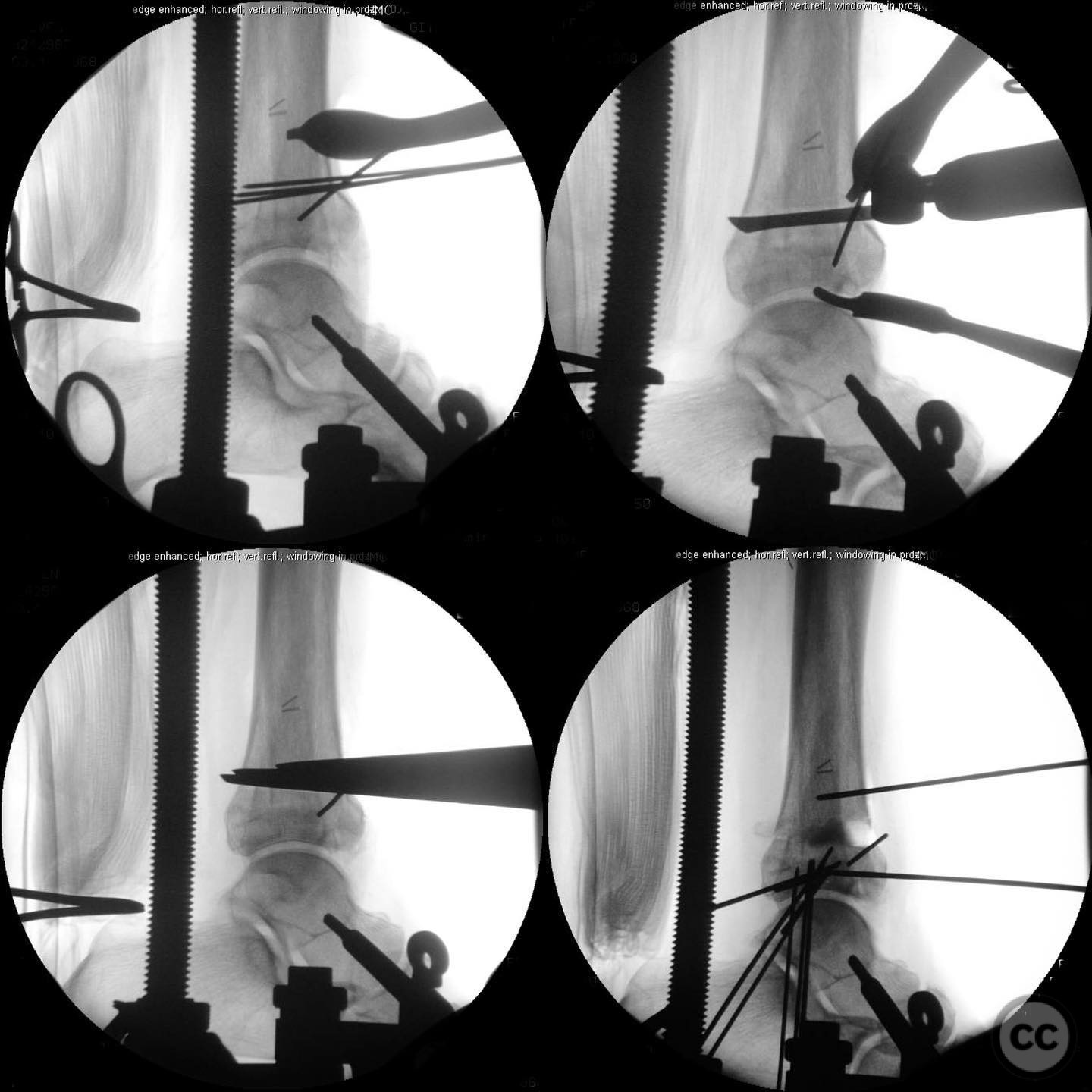
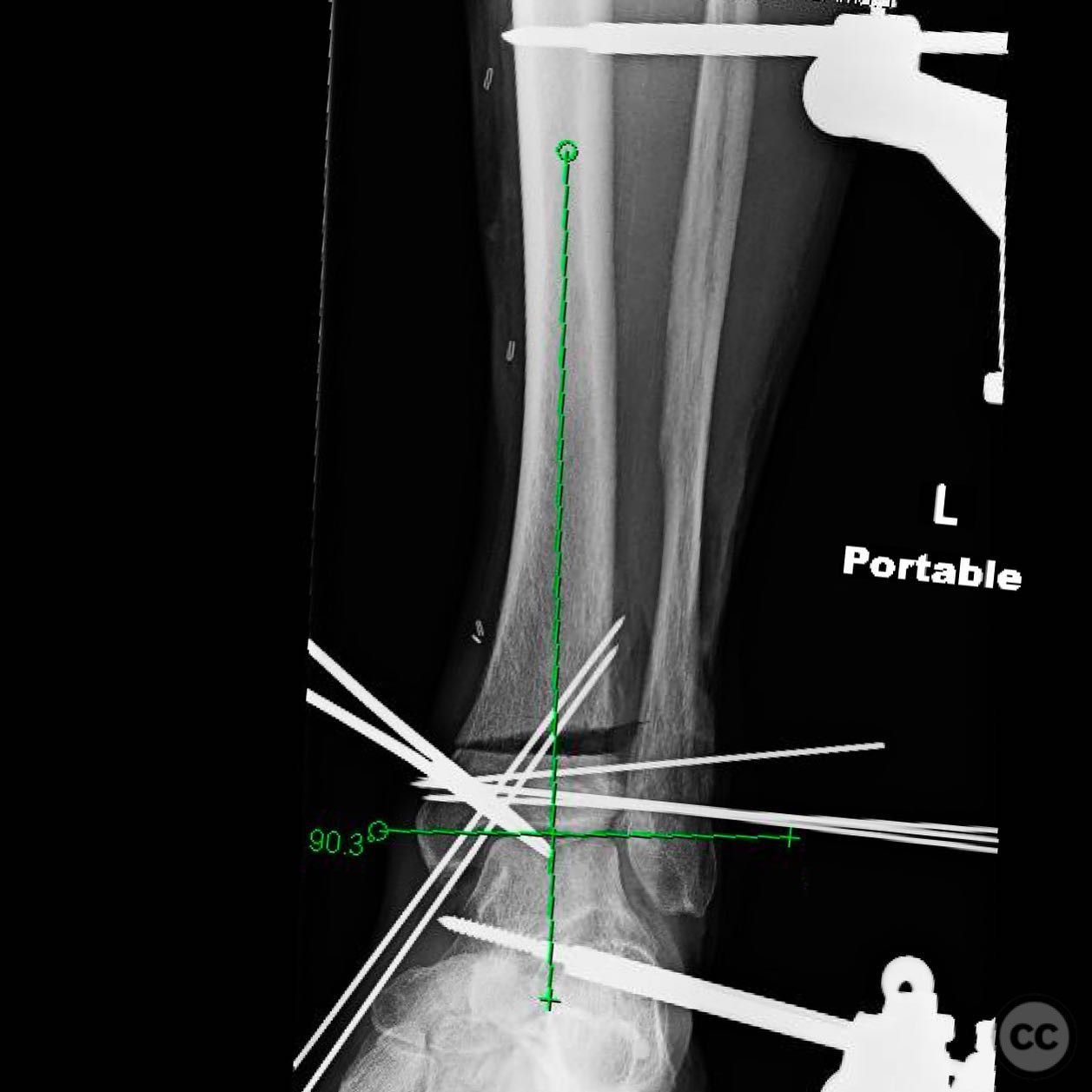
Anatomical surgical approach: A longitudinal anterolateral approach was utilized, allowing for lateral distraction and exposure of the distal tibia. The osteotomy was guided by K-wires, maintaining a medial hinge. Structural grafting was performed using both structural graft and autograft material, followed by compression and fixation with a locking plate.
Operative remarks:The surgeon emphasized the importance of preoperative planning, including vascular assessment and ensuring supple lateral skin to accommodate surgical manipulation. The procedure required meticulous execution of a supramalleolar opening wedge osteotomy to correct the malunion, followed by precise restoration of fibular length to achieve stable fixation. The patient was informed of the potential risks and uncertain outcomes due to the chronicity of the injury and underlying neuropathy.
Postoperative protocol: Postoperative rehabilitation included protected weight-bearing with gradual progression as tolerated, emphasizing compliance with follow-up appointments and monitoring for potential complications related to diabetes and neuropathy.
Follow up: Not specified.
Orthopaedic implants used: Lateral distractor, K-wires, structural graft, autograft, locking plate.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 337 times
14 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Supramalleolar Osteotomy for Distal Tibia and Fibula Malunion in a Diabetic Patient with Peripheral Neuropathy. Journal of Orthopaedic Surgery and Traumatology. Case Report 2631920 Published Online Jul 14 2025.