

Percutaneous CurvaFix Fixation for Pelvic Ring Instability with Sacral and Contralateral Pubic Ramus Fractures
Score and Comment on this Case
Clinical Details
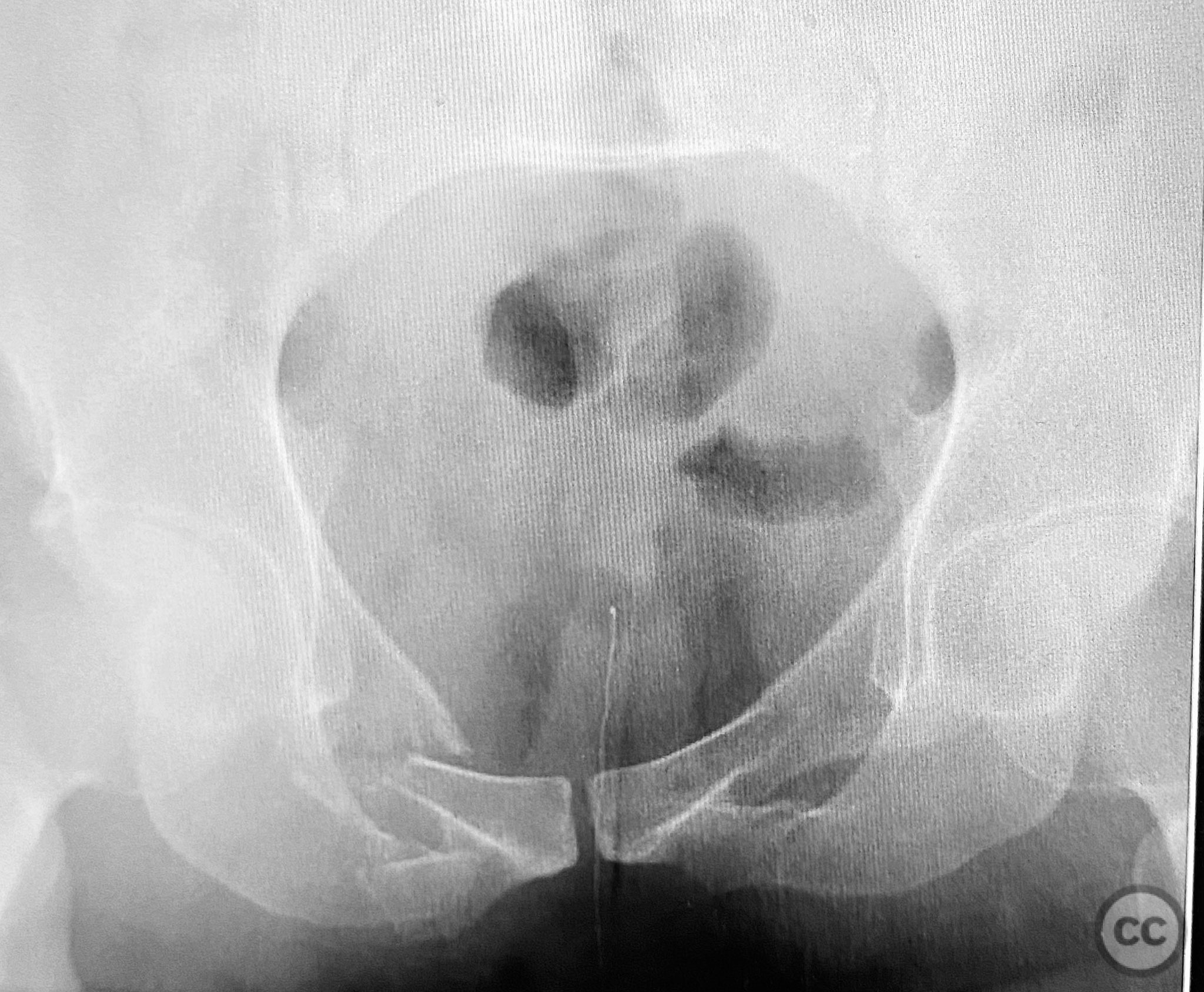
Clinical and radiological findings: A patient presented with pelvic ring instability and deformity secondary to a left sacral fracture and a right pubic ramus fracture. Imaging demonstrated a displaced left sacral fracture (AO/OTA 61-C1.3) and a right superior pubic ramus fracture, with associated pelvic ring deformity. No neurovascular compromise was noted on initial assessment.
Preoperative Plan
Planning remarks: The preoperative plan was for closed manipulative reduction of the pelvic ring under fluoroscopic guidance, followed by percutaneous fixation of the right pubic ramus fracture and stabilization of the pelvic ring deformity using a CurvaFix intramedullary device. No open approaches were planned.
Surgical Discussion
Patient positioning: The patient was positioned supine on a radiolucent table to facilitate intraoperative fluoroscopic imaging of the pelvis in multiple planes.
Anatomical surgical approach: A percutaneous approach was utilized. After standard preparation and draping, a small incision was made over the entry point of the right superior pubic ramus. The near cortex was prepared in routine fashion. A curved guide was introduced along the intramedullary pathway of the superior pubic ramus, followed by measurement of required device length. Sequential reaming was performed: first with an opening reamer, then with a pathway reamer to accommodate the device trajectory. The insertion guide wire was exchanged into position, and the CurvaFix device was inserted along the prepared pathway. The device was then locked to achieve rigid fixation.
Operative remarks:The application of the CurvaFix device was straightforward. Preparation of the near pathway, insertion of the curved guide, length measurement, reaming, and device insertion proceeded without technical difficulty. The device demonstrated rigid fixation upon locking, even in the presence of comminution at the fracture site.
Postoperative protocol: Postoperatively, the patient was maintained toe-touch weight bearing on the affected side for 6 weeks, with progressive advancement to full weight bearing as tolerated thereafter. Early mobilization with physiotherapy was initiated to preserve hip and knee range of motion.
Follow up: Not specified
Orthopaedic implants used: CurvaFix 130mm length / 7.5mm diameter intramedullary device
Search for Related Literature


Industry Sponsership
contact us for advertising opportunities
Article viewed 303 times
11 Sep 2025
Add to Bookmarks
Full Citation
Cite this article:
Routt, ML. (2025). Percutaneous CurvaFix Fixation for Pelvic Ring Instability with Sacral and Contralateral Pubic Ramus Fractures. Journal of Orthopaedic Surgery and Traumatology. Case Report 26050777 Published Online Sep 11 2025.