



 articular incongruity._3.jpg)
 articular incongruity._4.jpg)
 articular incongruity._5.jpg)
 articular incongruity._6.jpg)
 articular incongruity._7.jpg)
 articular incongruity._2.jpg)
 articular incongruity. (.jpg)
 articular incongruity._1.jpg)
Glenoid Fracture with Scapular Body Involvement in a Young Active Male
Score and Comment on this Case
Clinical Details
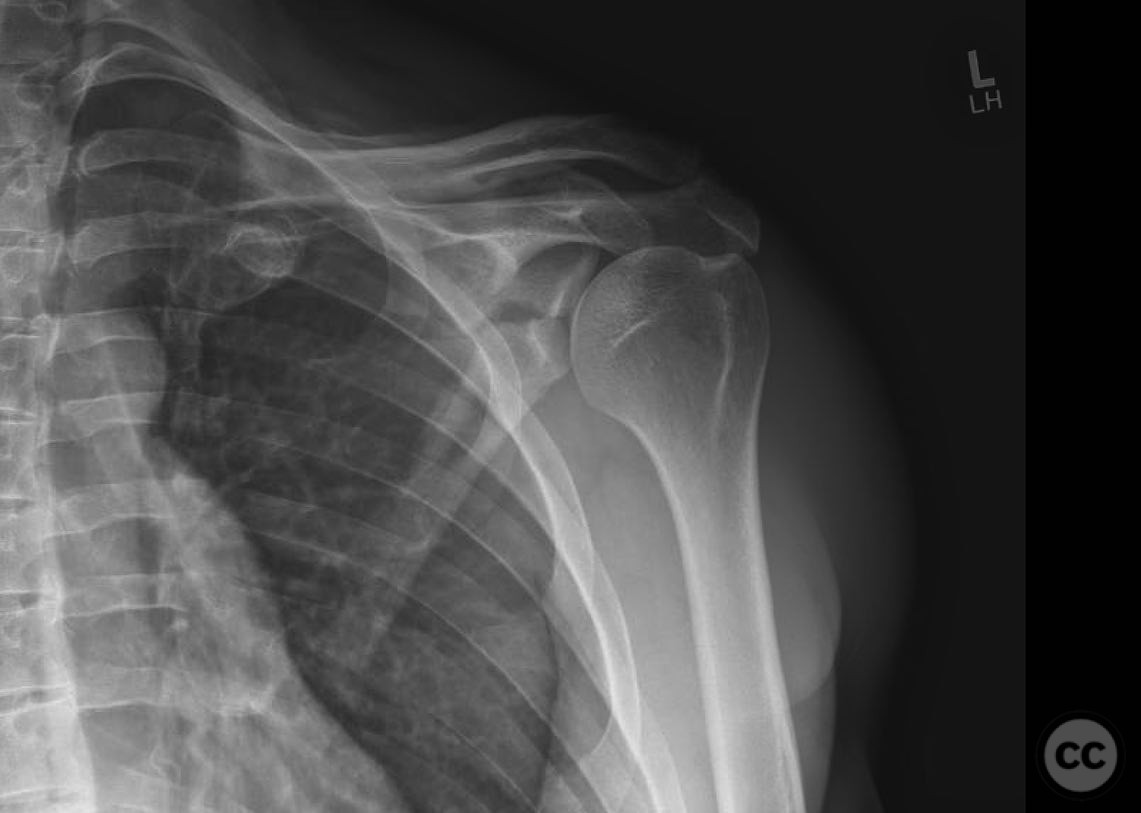
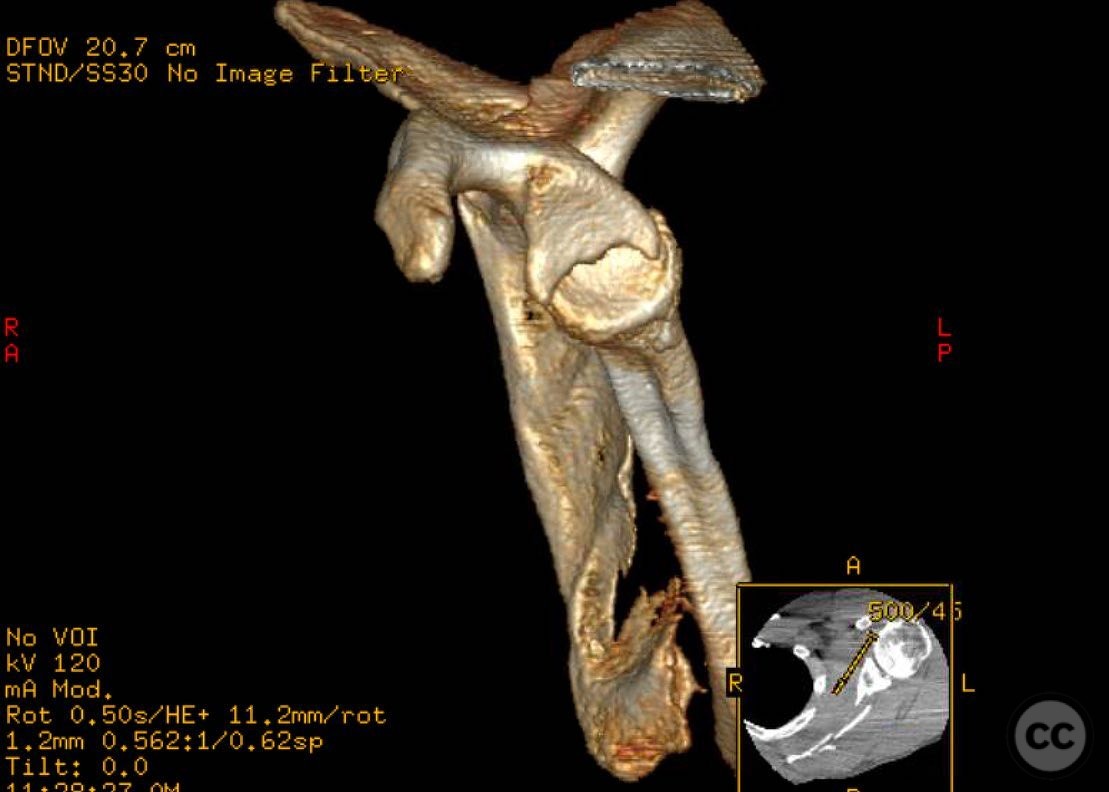
Clinical and radiological findings: The patient is a young, extremely fit, and active male, presenting with a scapular fracture involving the glenoid. Radiographic evaluation indicated articular incongruity, with a glenopolar angle less than 22 degrees as measured on the Grashy view. The scapular body demonstrated lateralization greater than 2 cm, also assessed on the Grashy view. Angulation of the scapular body was significant on the scapular Y view. These findings, combined with the patient's high activity level and long-term functional demands, warranted surgical intervention.
Preoperative Plan
Planning remarks: The preoperative plan involved a modified Judet approach to address the glenoid fracture. A "window" was planned at the glenoid fracture site through the infraspinatus muscle belly to facilitate manipulation and reduction. Careful attention was given to the suprascapular nerve and artery located at the spinoglenoid notch.
Surgical Discussion
Patient positioning: The patient was positioned laterally to optimize intraoperative imaging and access to the surgical site.
Anatomical surgical approach: A modified Judet approach was utilized, involving an incision over the posterior aspect of the shoulder. Dissection proceeded through the deltoid and infraspinatus muscles, creating an interval between the teres minor and infraspinatus tendons. An arthrotomy was performed between these tendons to address labral delamination and facilitate reduction of the glenoid fracture.
Operative remarks:The reduction was particularly challenging due to partial delamination and bowstringing of the labrum, complicating joint congruity restoration. Precise anatomical knowledge was crucial to avoid injury to the suprascapular nerve and artery during exposure and reduction maneuvers.
Postoperative protocol: Postoperative rehabilitation included immobilization in a sling for initial weeks, followed by gradual passive range of motion exercises. Active range of motion and strengthening exercises were introduced progressively based on clinical and radiographic healing.
Follow up: Not specified.
Orthopaedic implants used: Orthopaedic implants used included plates and screws for stabilization of the glenoid and scapular body fractures.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 337 times
16 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Glenoid Fracture with Scapular Body Involvement in a Young Active Male. Journal of Orthopaedic Surgery and Traumatology. Case Report 24978364 Published Online Jul 16 2025.