




Bony PCL Avulsion with Partial LCL Rupture
Score and Comment on this Case
Clinical Details
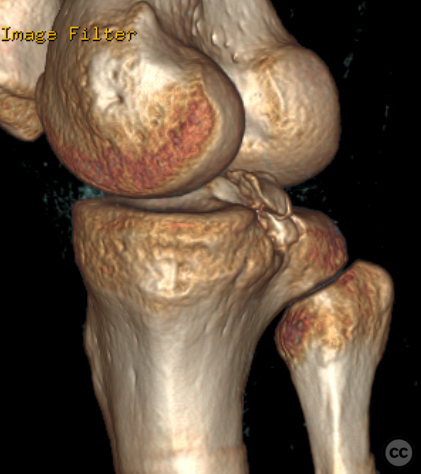
Clinical and radiological findings: A 30-year-old male sustained a fall from a height of over 2 meters, resulting in a posterior cruciate ligament (PCL) bony avulsion and a partial rupture of the lateral collateral ligament (LCL) on the femoral side. The patient exhibited posterior instability but no varus instability, which was confirmed under anesthesia. The LCL was deemed stable and managed conservatively in parallel with postoperative rehabilitation of the PCL injury.
Preoperative Plan
Planning remarks: The planned surgical approach involved a posterior incision to access the bony avulsion of the PCL.
Surgical Discussion
Patient positioning: The patient was positioned prone on a radiolucent operating table, allowing access to the posterior aspect of the right leg with approximately 15 degrees of passive flexion. The left leg was lowered out of the way to facilitate lateral fluoroscopic imagin
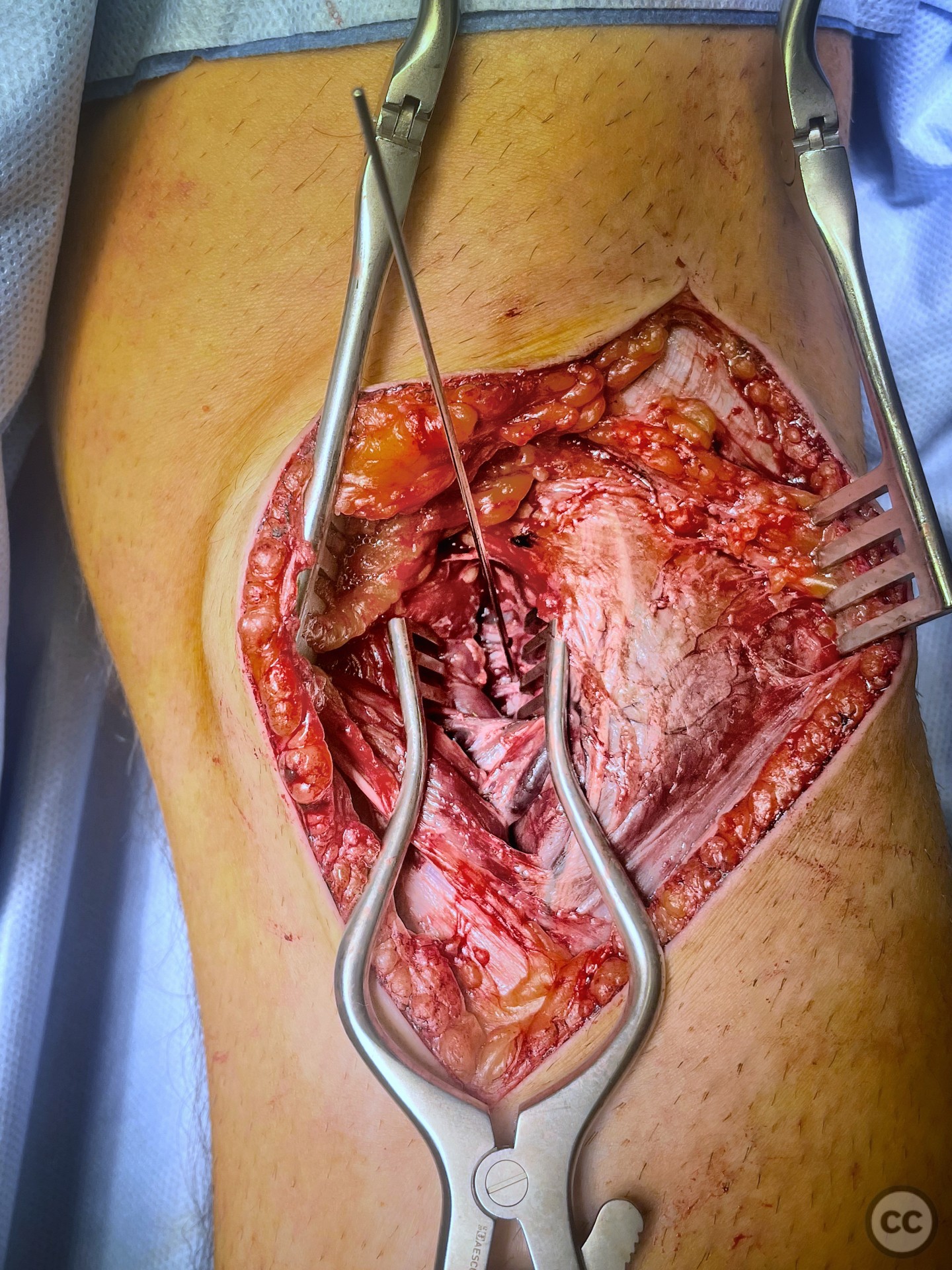
Anatomical surgical approach: An S-shaped incision was made, curving from laterally to distally medially across the flexion crease of the knee. Subcutaneous dissection identified the superficial saphenous vein. The fascia overlying the medial aspect of the neurovascular bundle was incised to identify the popliteal vessels and the posterior tibial nerve. Blunt dissection proceeded medially to the neurovascular bundle, lateral to the medial head of gastrocnemius, reaching up to the level of the posterior tibial plateau. The middle genicular artery was mobilized proximally, allowing direct access to the bony footprint of the PCL and its avulsion.
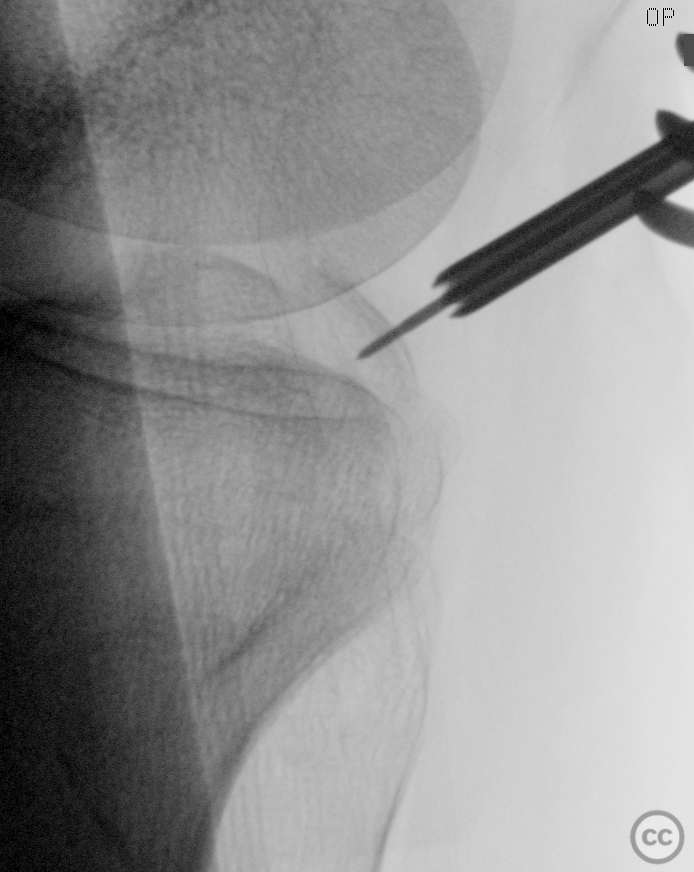
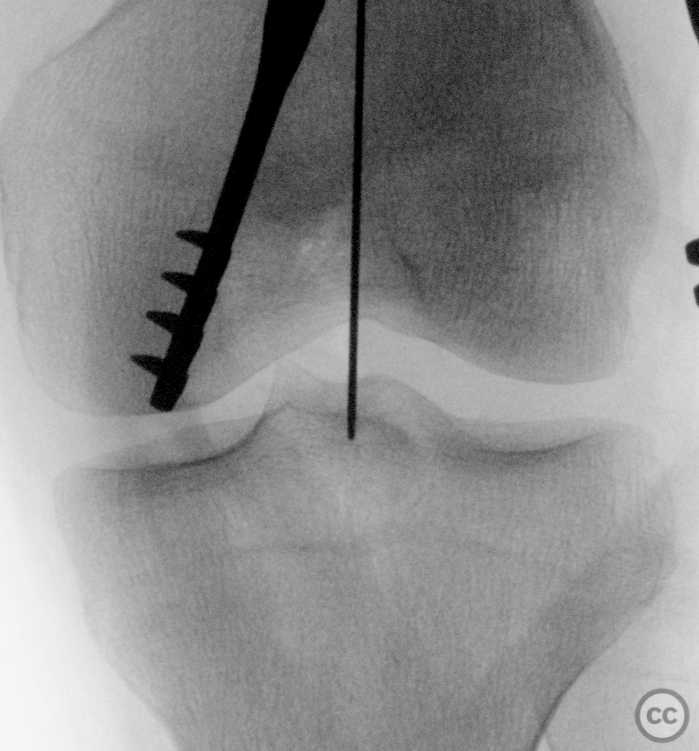
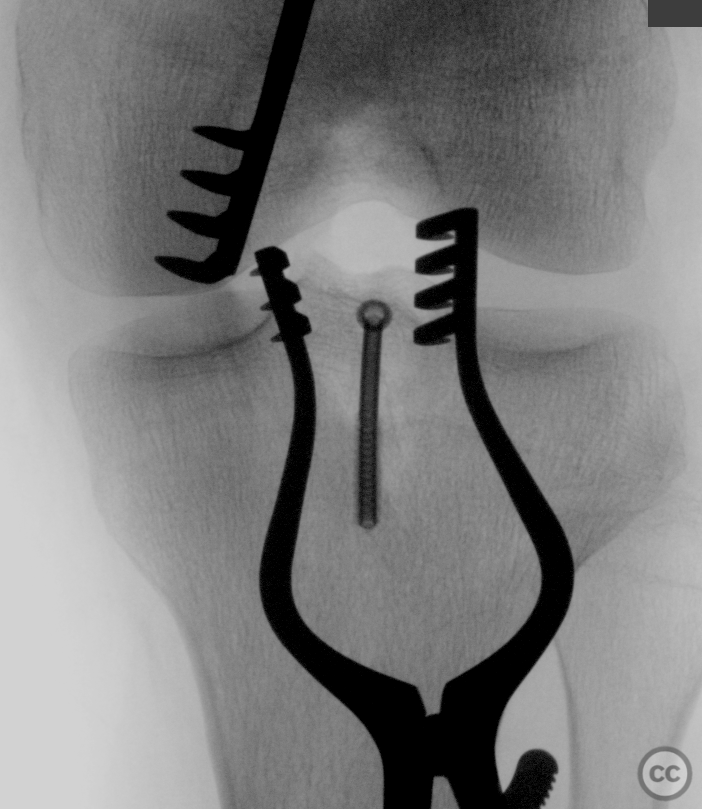
Operative remarks:Gentle elevation and mobilization under fluoroscopic guidance were followed by reduction of the fragment and provisional fixation using a 1.6-millimeter K-wire under multiplanar fluoroscopic control. Following minor adjustments and confirmation of fracture reduction, a 4.0-millimeter cannulated screw was introduced over a K-wire through the middle of the fragment, achieving excellent purchase, reduction, and compression. Multiplex fluoroscopy confirmed final screw positioning following removal of all K-wires. Deflation of the tourniquet allowed examination for any vascular injury, confirming no active bleeding.
Postoperative protocol: M4S knee orthosis.
Follow up: Not specified
Orthopaedic implants used: 4.0-millimeter cannulated screw
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 795 times
03 Jun 2024
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2024). Bony PCL Avulsion with Partial LCL Rupture. Journal of Orthopaedic Surgery and Traumatology. Case Report 24933772 Published Online Jun 03 2024.