








Capitellum and Radial Head Fracture with Trochlear Involvement
Score and Comment on this Case
Clinical Details
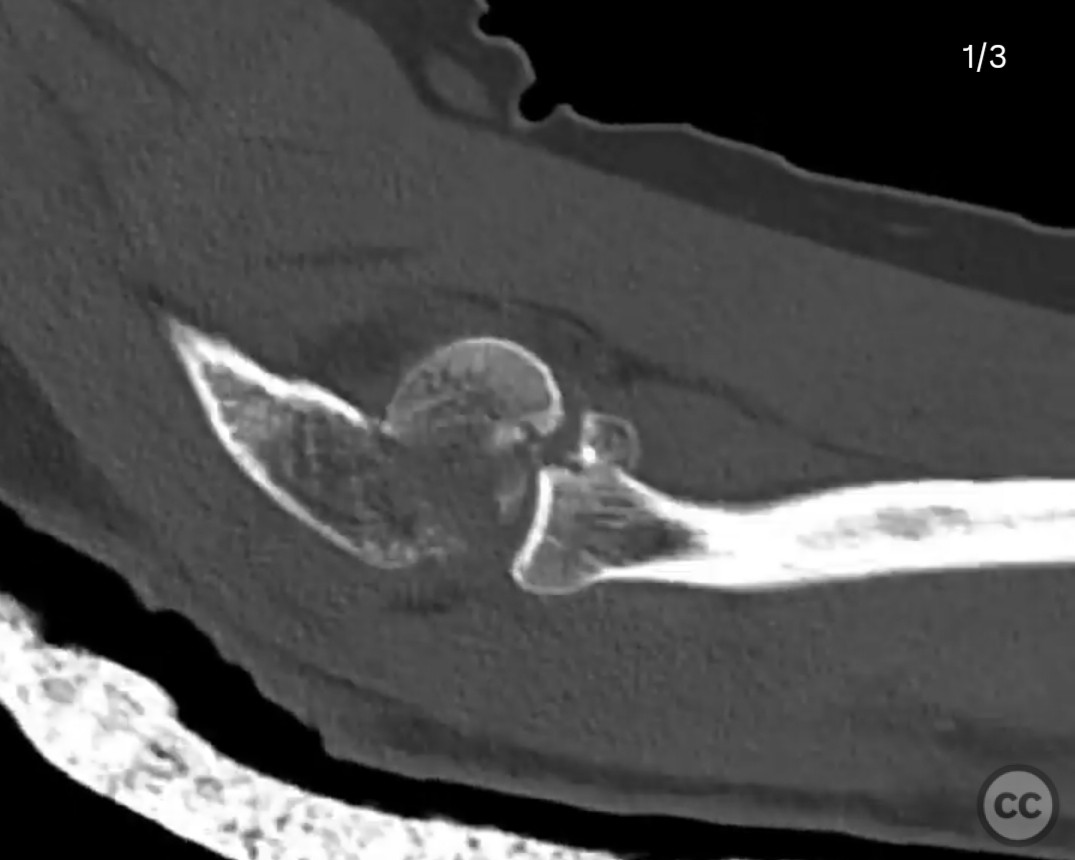
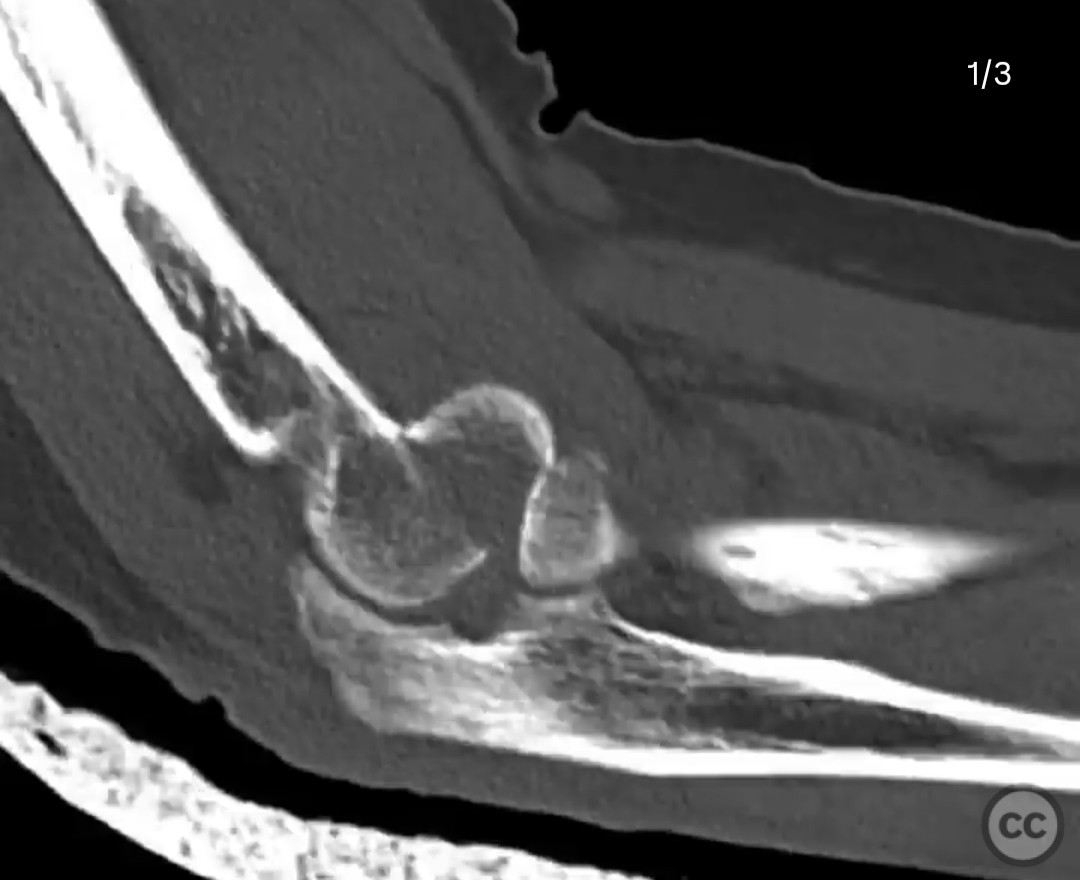
Clinical and radiological findings: A 61-year-old patient presented following a fall, with significant pain and swelling localized to the elbow. Radiographic evaluation revealed a shear fracture of the capitellum with minor trochlear involvement, accompanied by a radial head fracture. The injury was closed, and initial management in the emergency department included an attempt at closed reduction using extension, varus force, and pressure on the fragment followed by flexion.
Preoperative Plan
Planning remarks: The preoperative plan involved an open reduction and internal fixation via a Kocher approach. Given the fracture pattern, visualization and implant placement were prioritized. The plan included surgically destabilizing the elbow to facilitate reduction and allow for screw placement perpendicular to the fracture line.
Surgical Discussion
Patient positioning: The patient was positioned supine with the affected arm on an arm table, allowing for adequate access to the lateral aspect of the elbow.
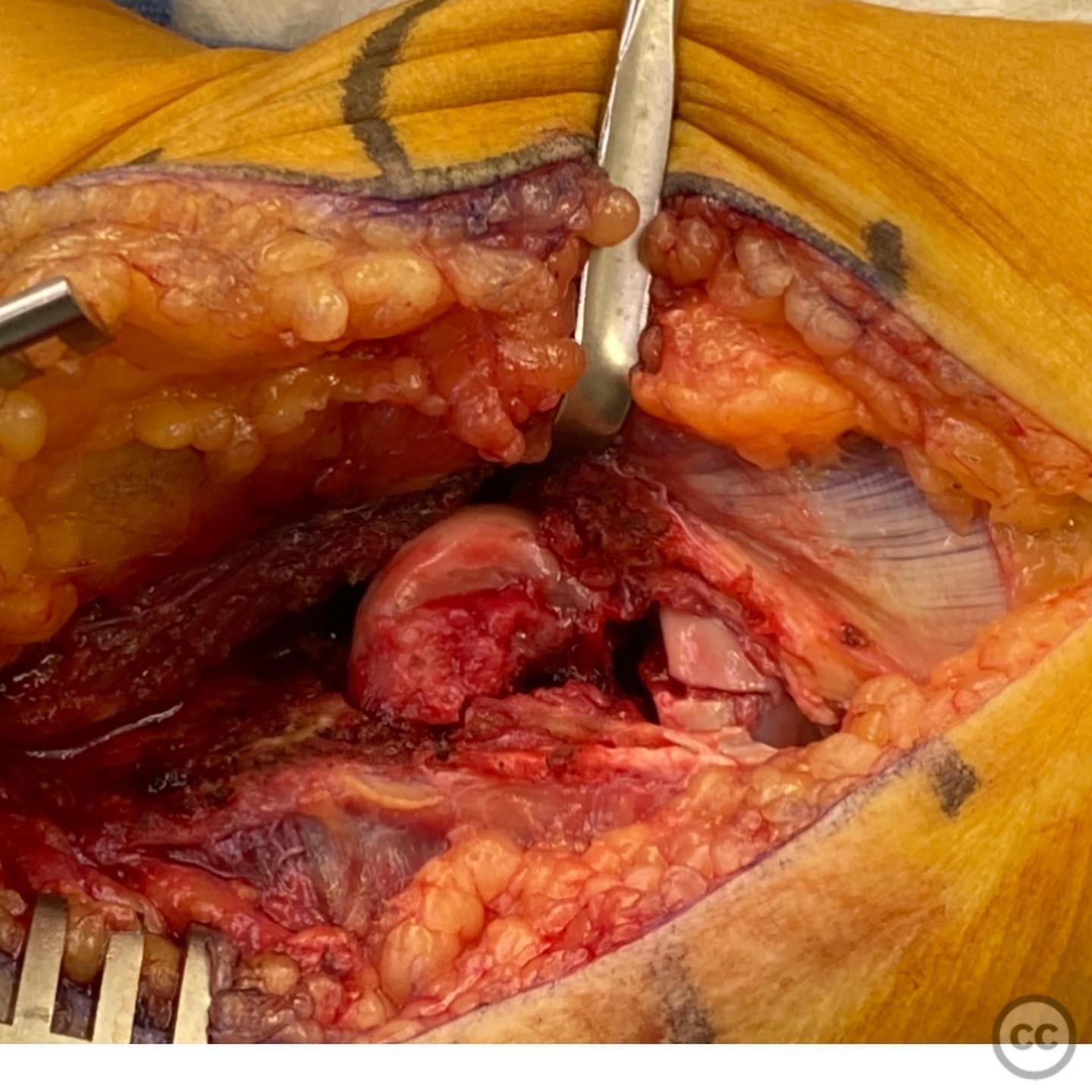
Anatomical surgical approach: A Kocher approach was utilized, involving an incision over the lateral aspect of the elbow. The common extensor origin and anterior capsule were elevated as a sleeve while preserving the lateral ulnar collateral ligament (LUCL) to maintain elbow stability. This approach provided access to the capitellum and trochlea for fracture reduction and fixation.
Operative remarks:Intraoperatively, anterior-to-posterior countersunk 2.0 mm lag screws were used for fixation of the capitellum fracture, supplemented by orthogonal screws for additional stability. The radial head fracture was repaired using 1.5 mm and 1.3 mm screws. A double-loaded suture anchor was employed to reattach the common extensor origin. Careful assessment of elbow range of motion was performed post-fixation to ensure no impingement or instability.
Postoperative protocol: Postoperatively, the patient was immobilized in a splint for one week, followed by transition to a thermoplastic removable splint. A motion protocol was initiated thereafter to restore range of motion while protecting the repair.
Follow up: Not specified
Orthopaedic implants used: 2.0 mm lag screws, 1.5 mm and 1.3 mm screws, double-loaded suture anchor.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 356 times
13 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Capitellum and Radial Head Fracture with Trochlear Involvement. Journal of Orthopaedic Surgery and Traumatology. Case Report 24134318 Published Online Jul 13 2025.