_0.jpg)
_1.jpg)








Rotational Ankle Fracture Dislocation with Double Oblique Fibular Fracture
Score and Comment on this Case
Clinical Details
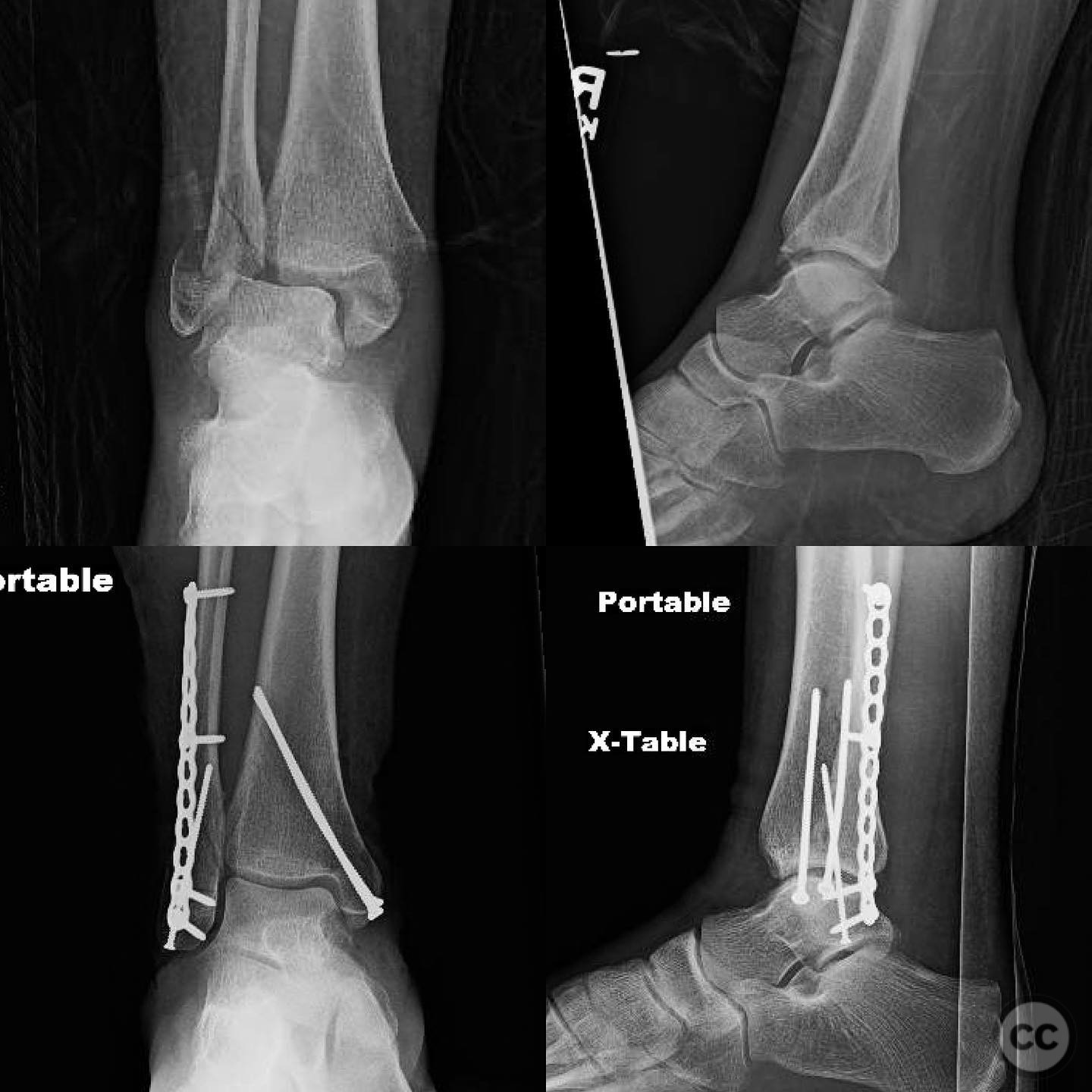
Clinical and radiological findings: A patient presented with a rotational ankle fracture dislocation. Initial radiographs and a CT scan were obtained to assess the injury pattern, revealing a double oblique fibular fracture with a middle segment involving the anterior inferior tibiofibular ligament (AITFL) origin, and an avulsion of the posterior inferior tibiofibular ligament (PITFL) without posterior dislocation. The contralateral ankle was imaged for intraoperative reference to assist in syndesmosis evaluation.
Preoperative Plan
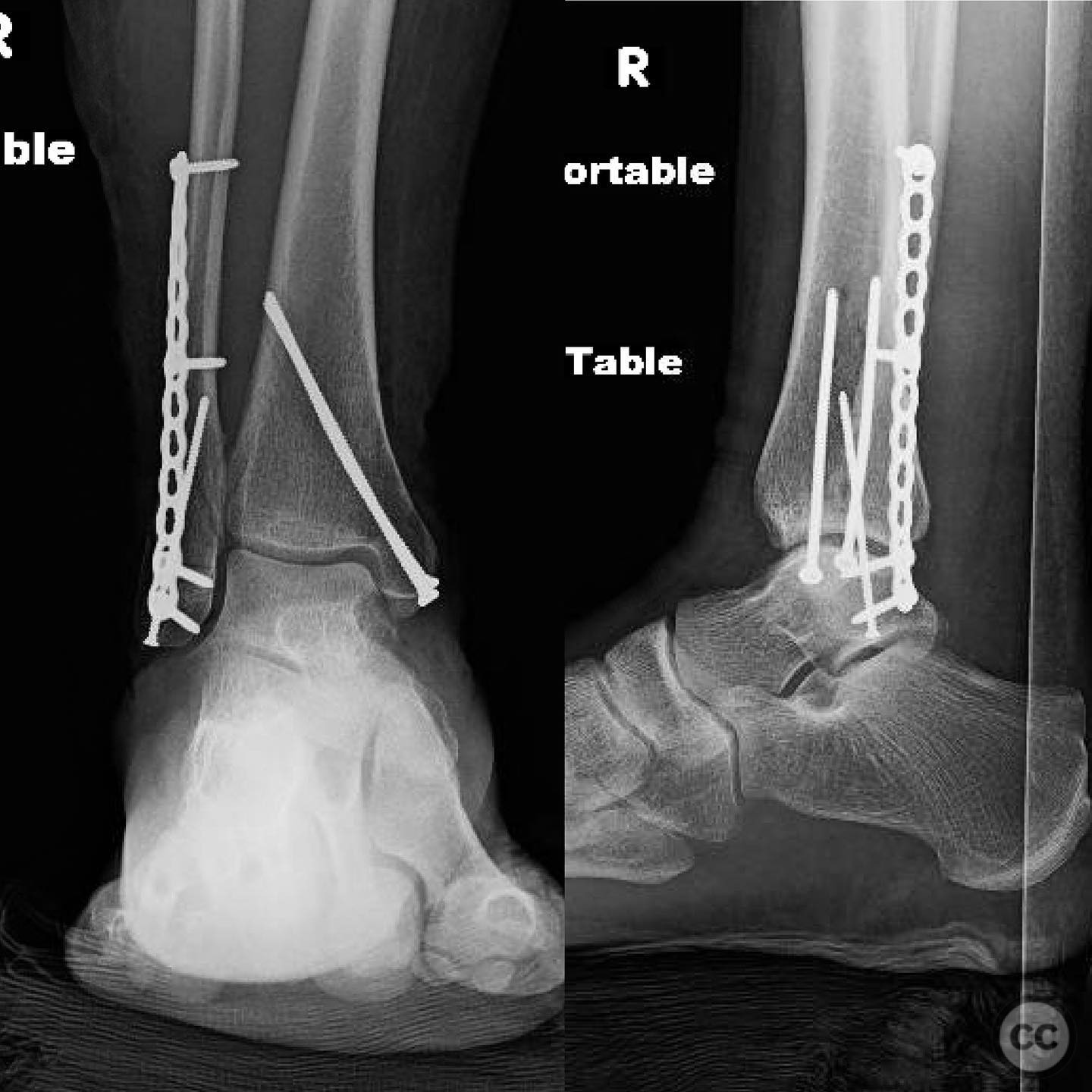
Planning remarks: The preoperative plan included a posterolateral approach to the fibula for fixation of the double oblique fracture pattern, with fragment-specific fixation anticipated due to the involvement of the AITFL origin. An open reduction of the medial malleolus was also planned, with fixation using screws.
Surgical Discussion
Patient positioning: The patient was positioned supine on the operating table.
Anatomical surgical approach: A posterolateral approach to the fibula was utilized, allowing for direct access to the fracture site. Sequential clamping was performed, followed by fixation using two 2.4mm lag screws due to the matching obliquity of the fracture. An additional anti-glide screw was placed for neutralization. The medial malleolus was approached directly, reduced with a straight curved modified clamp, and fixed with 2.7mm screws.
Operative remarks:Intraoperative stress testing of the syndesmosis was conducted, including coronal plane (Cotton test), sagittal plane, and rotational stability assessments. No evidence of syndesmotic instability was found post-fixation on any examination. The importance of identifying "occult" syndesmosis instability was noted, though no additional stabilization was deemed necessary in this case.
Postoperative protocol: Postoperative rehabilitation included protected weight-bearing with gradual progression based on clinical and radiographic healing.
Follow up: Not specified.
Orthopaedic implants used: 2.4mm lag screws, 2.7mm screws for medial malleolus fixation, anti-glide screw for fibular stabilization.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 288 times
14 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Rotational Ankle Fracture Dislocation with Double Oblique Fibular Fracture. Journal of Orthopaedic Surgery and Traumatology. Case Report 22762184 Published Online Jul 14 2025.