




Operative Management of Scapular and Glenoid Fractures via Modified Judet Approach
Score and Comment on this Case
Clinical Details
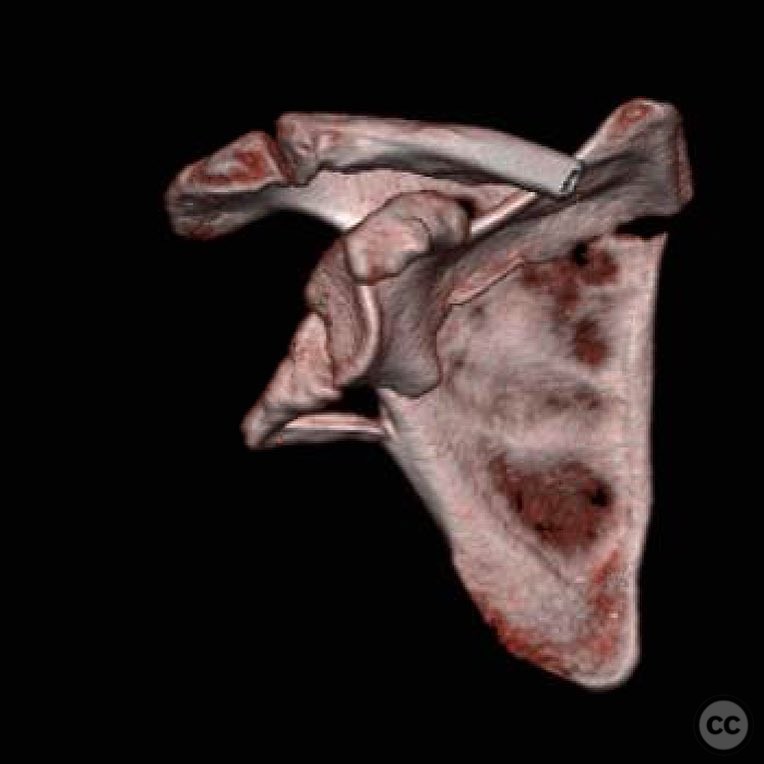
Clinical and radiological findings: A 44-year-old male sustained scapular and glenoid fractures following a high-energy collision between an all-terrain vehicle (ATV) and a truck on gravel backroads. Such injuries are relatively uncommon and typically associated with other serious non-orthopedic injuries due to the high-energy mechanism involved. The indication for surgical intervention in this case was articular involvement and associated displacement.
Preoperative Plan
Planning remarks: The preoperative plan involved an open reduction and internal fixation (ORIF) through a modified Judet approach, specifically utilizing the interval between the teres minor and infraspinatus muscles. The surgical strategy included reduction of the medial border, restoration of length along the lateral border using Schanz pins or a distractor, and stabilization of the glenoid with buttressing and coracoid screw placement.
Surgical Discussion
Patient positioning: Prone positioning was utilized for optimal access to the posterior aspect of the scapula and glenoid.
Anatomical surgical approach: The surgical approach was a modified Judet approach, involving a posterior incision with dissection through the interval between the teres minor and infraspinatus muscles. This provided direct access to the scapular body and glenoid neck for reduction and fixation.
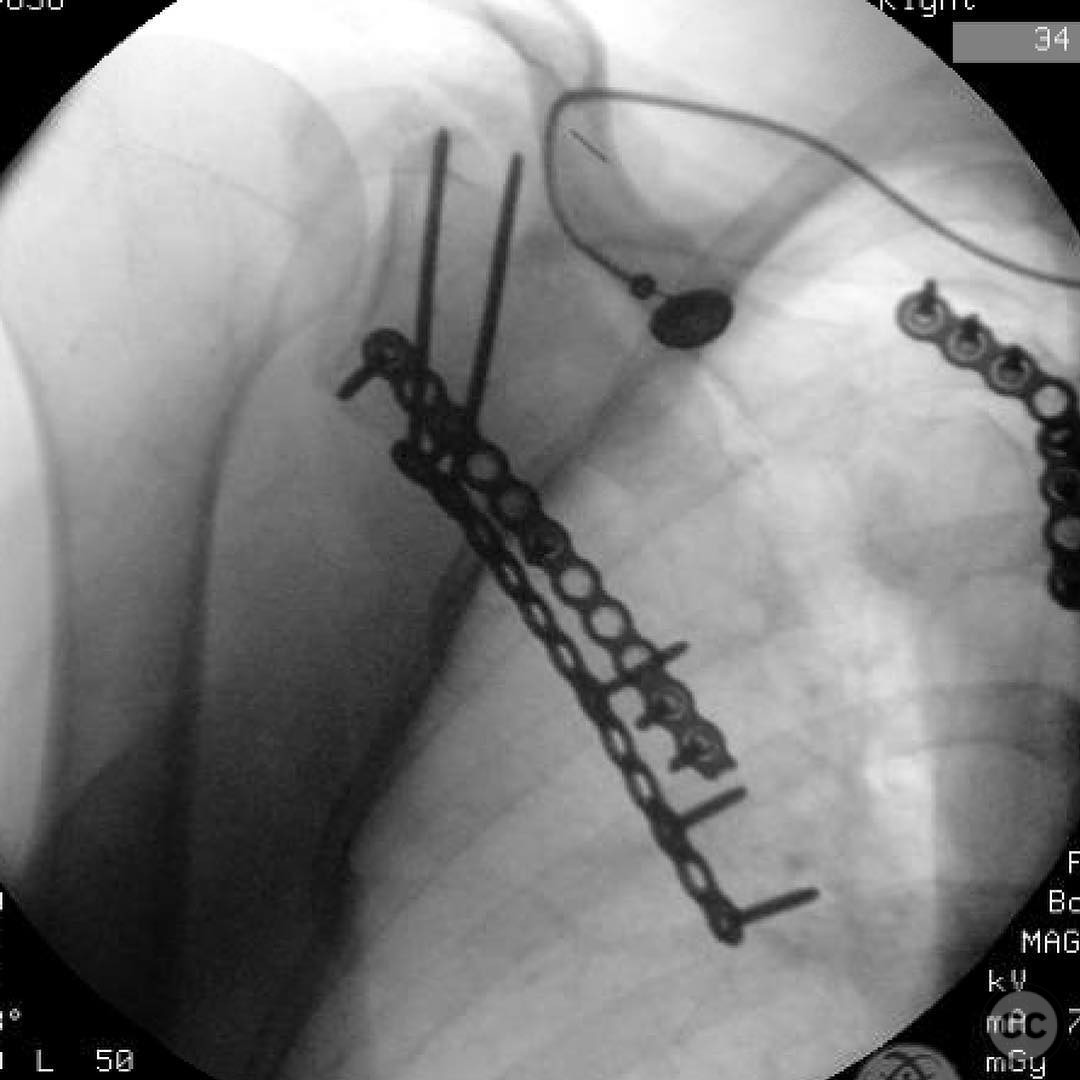
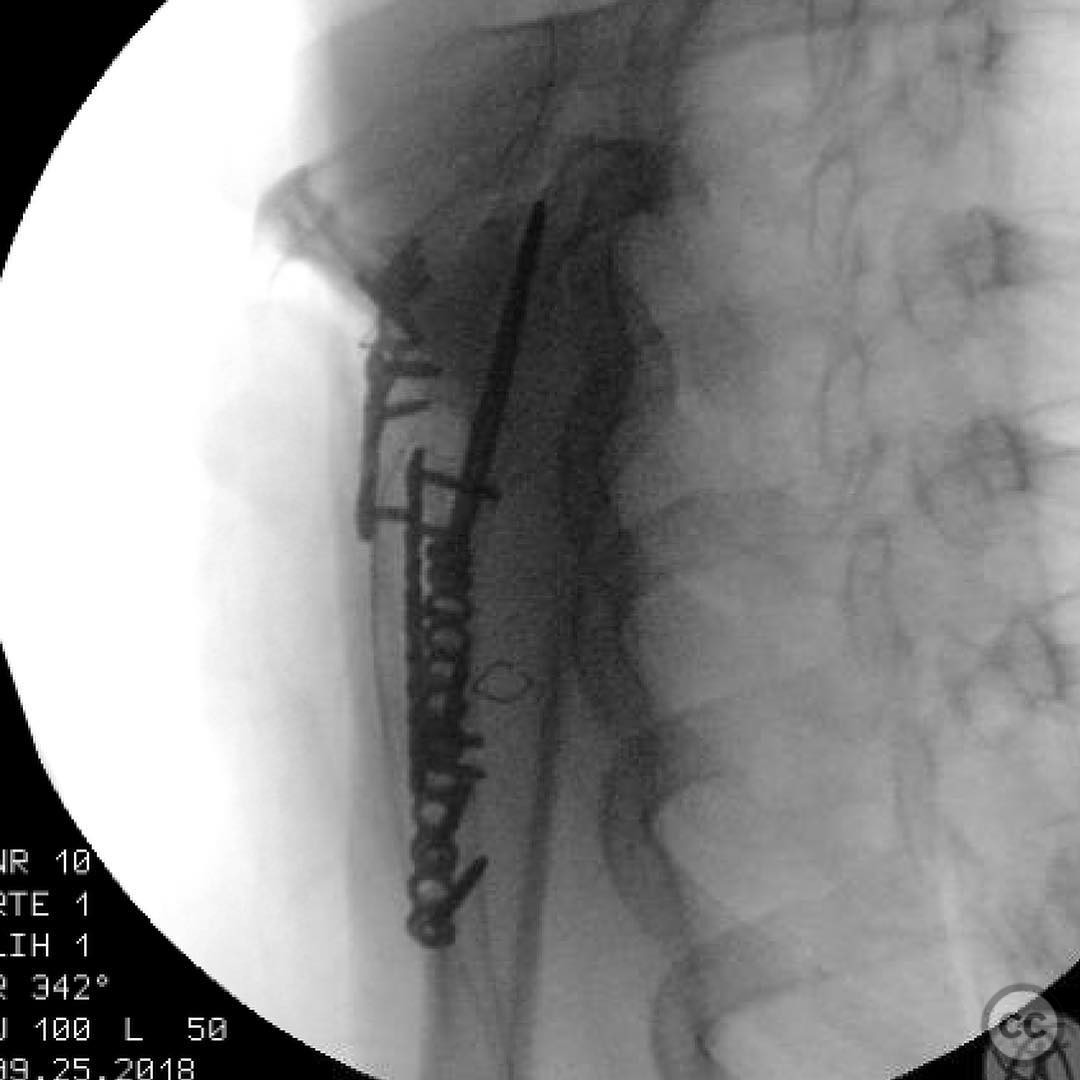
Operative remarks:The reduction process was algorithmic, beginning with the medial border of the scapula, which was retracted and stabilized using a flexible hinge technique. Length was restored along the lateral border with Schanz pins or a distractor. The glenoid neck was then aligned, buttressed, and secured with coracoid screws to ensure stability.
Postoperative protocol: Postoperative rehabilitation included early mobilization with passive range of motion exercises initiated immediately. Active-assisted range of motion exercises were introduced at 4 weeks, progressing to full active range of motion by 8 weeks. Strengthening exercises commenced at 12 weeks postoperatively.
Follow up: Not specified.
Orthopaedic implants used: Schanz pins, coracoid screws, buttress plate.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 390 times
25 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Operative Management of Scapular and Glenoid Fractures via Modified Judet Approach. Journal of Orthopaedic Surgery and Traumatology. Case Report 22094881 Published Online Jul 25 2025.