



Complete Posterior Facet Dislocation of the Calcaneus with Medial Wall Displacement.
Score and Comment on this Case
Clinical Details
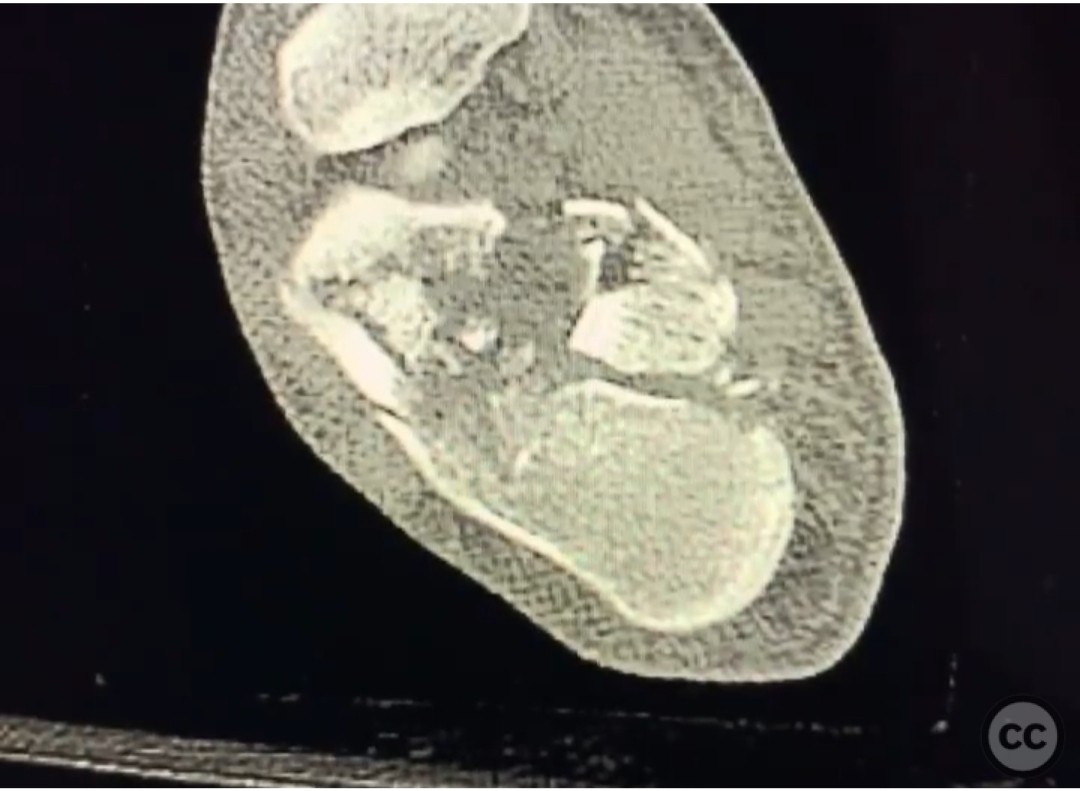
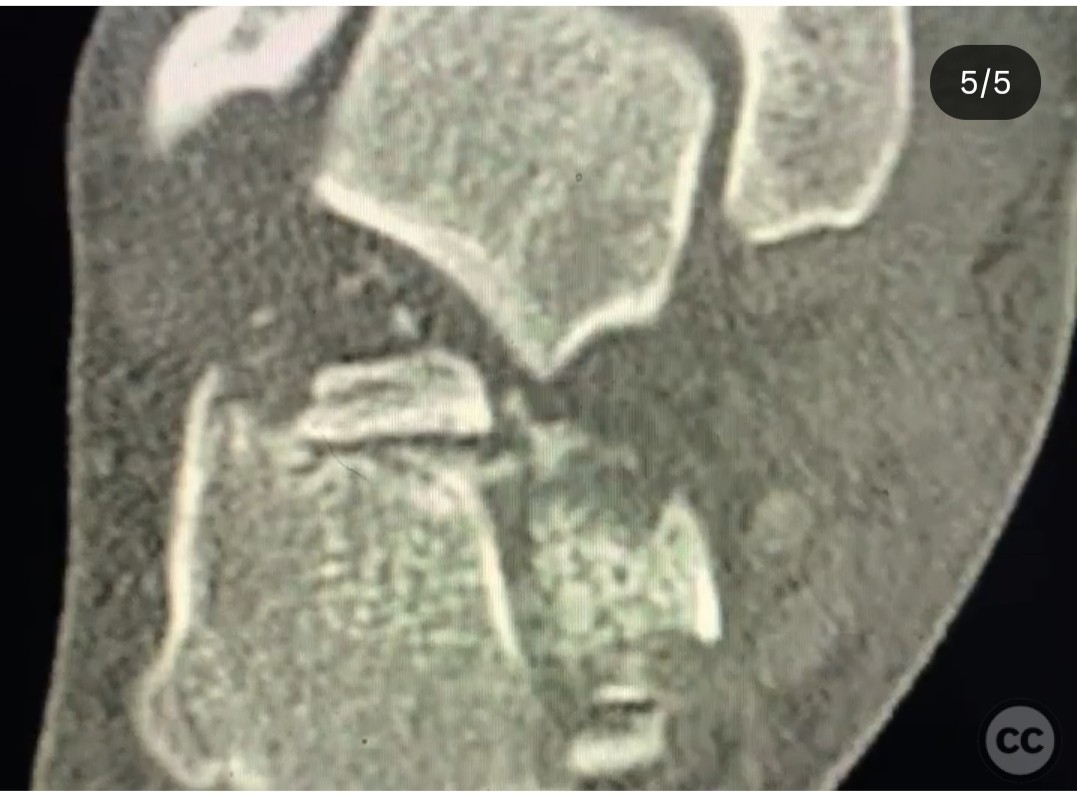
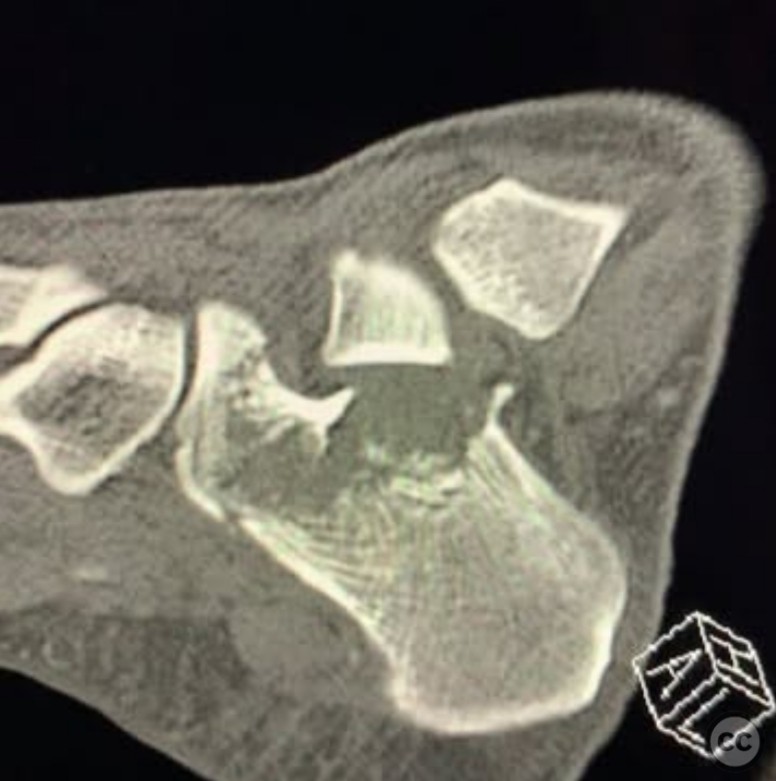
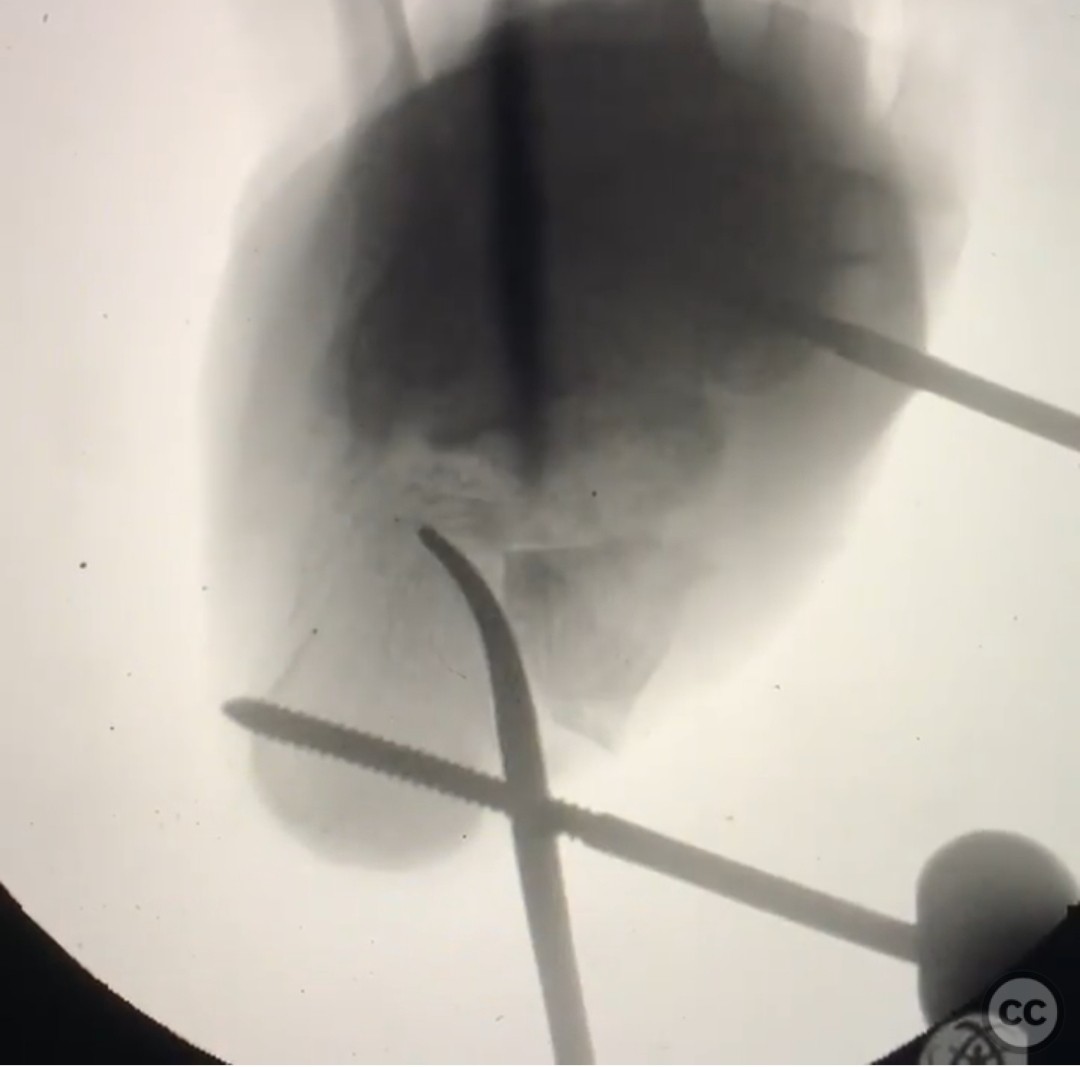
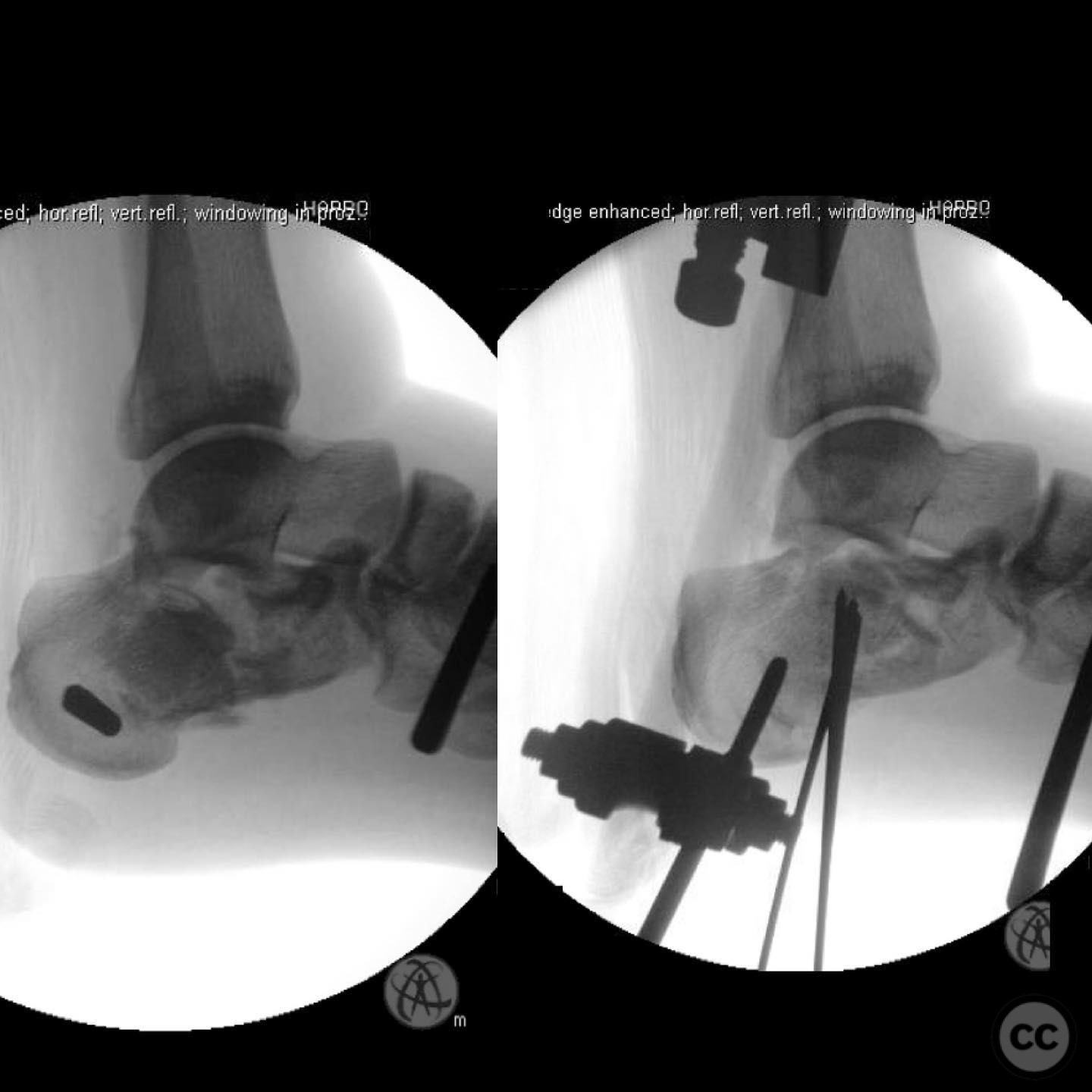
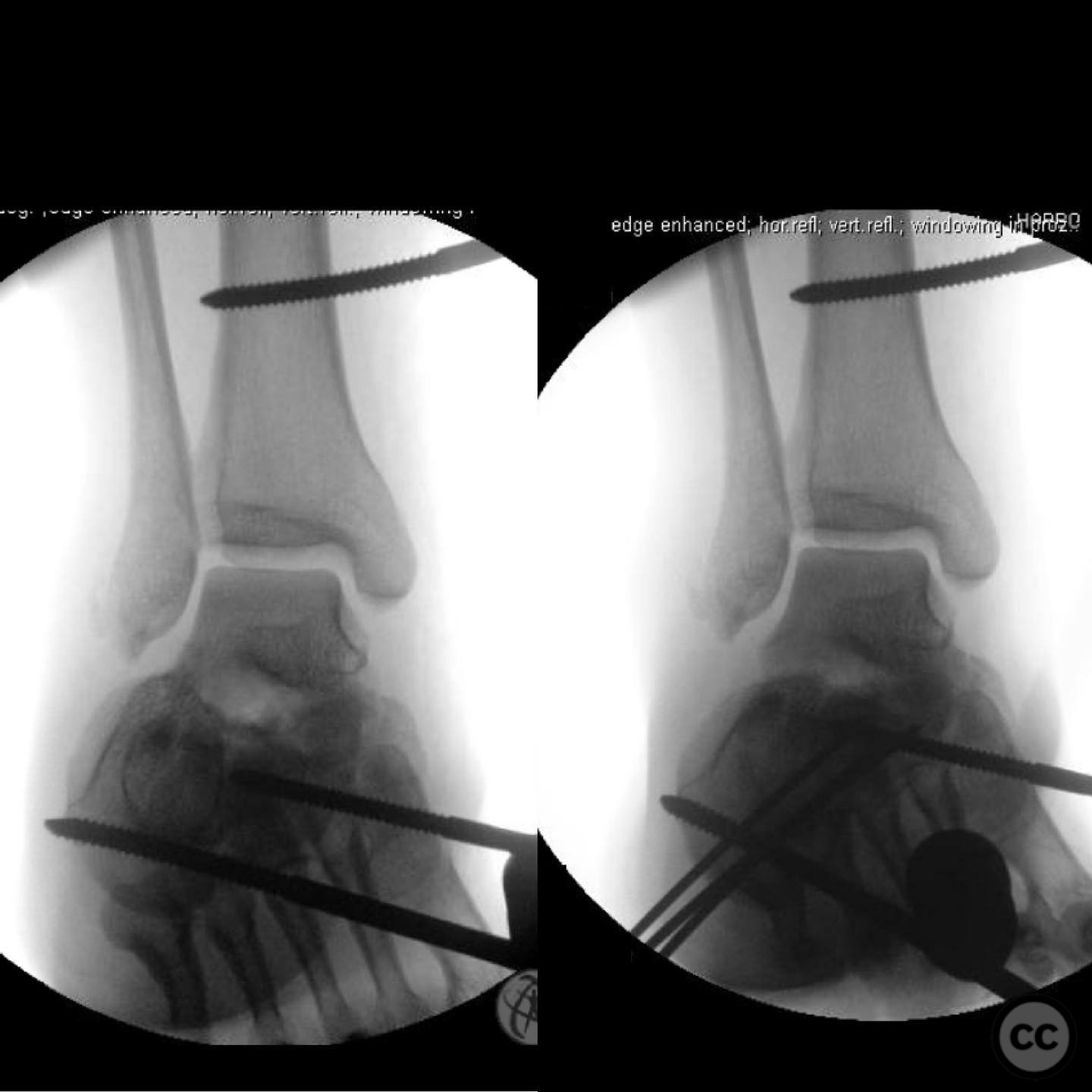
Clinical and radiological findings: A 31-year-old male sustained a fall from a height of 30 feet while climbing, resulting in a closed calcaneal fracture with medial blistering. The posterior tibial nerve was functioning but compromised. The patient also presented with a segmental fibular fracture and a femoral shaft fracture. No injuries to the spine, chest, or head were noted. Radiological assessment, including X-rays and CT scans, revealed a complete dislocation of the posterior facet of the calcaneus through the medial wall.
Preoperative Plan
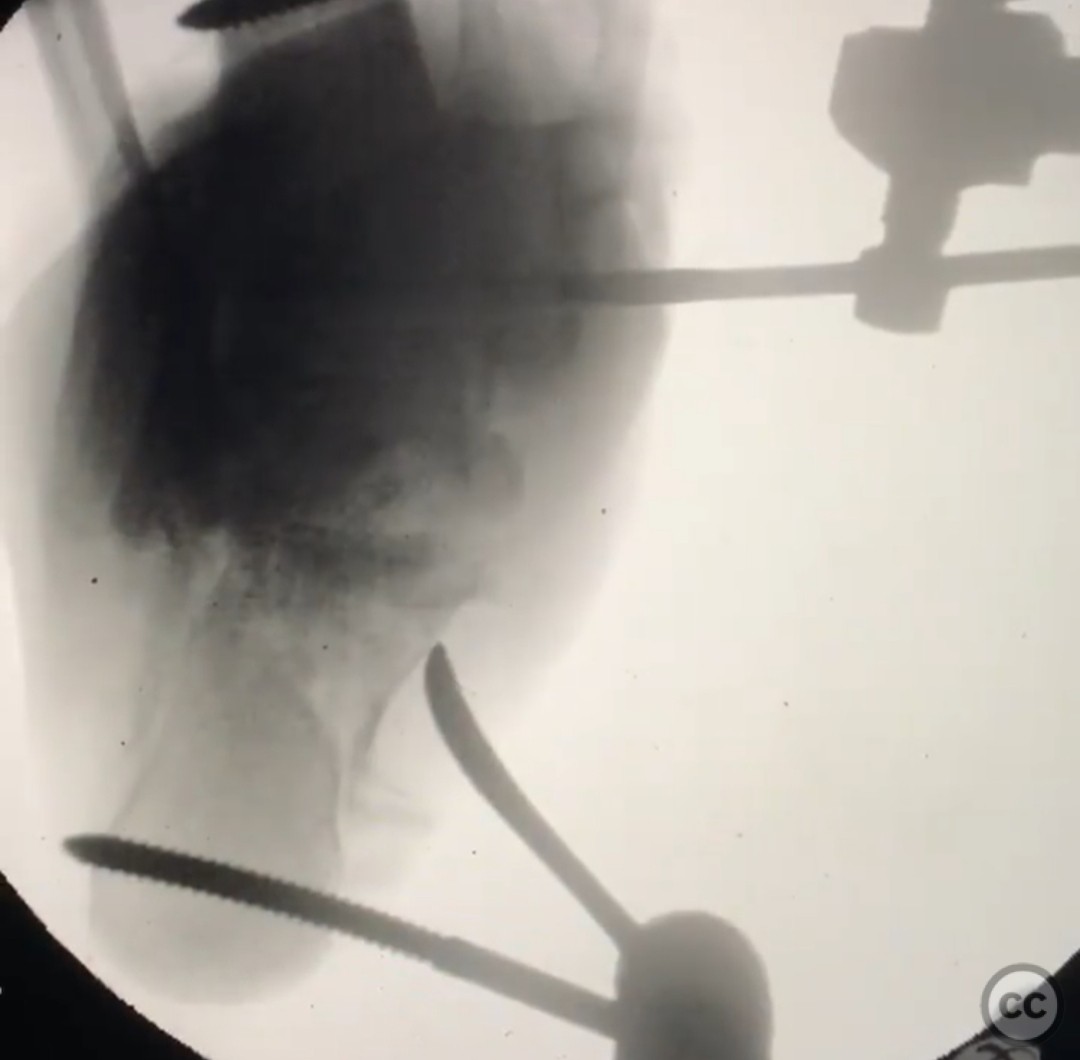
Planning remarks: The preoperative plan involved immediate reduction of the posterior facet to prevent skin necrosis. A medial external fixator was planned to distract and recreate length and height, allowing for reduction of the posterior facet. Percutaneous localization with a wire was planned, followed by reduction using instruments such as a joker, freer, or pusher.
Surgical Discussion
Patient positioning: Supine position with the affected limb elevated and supported to facilitate access to the medial aspect of the calcaneus.
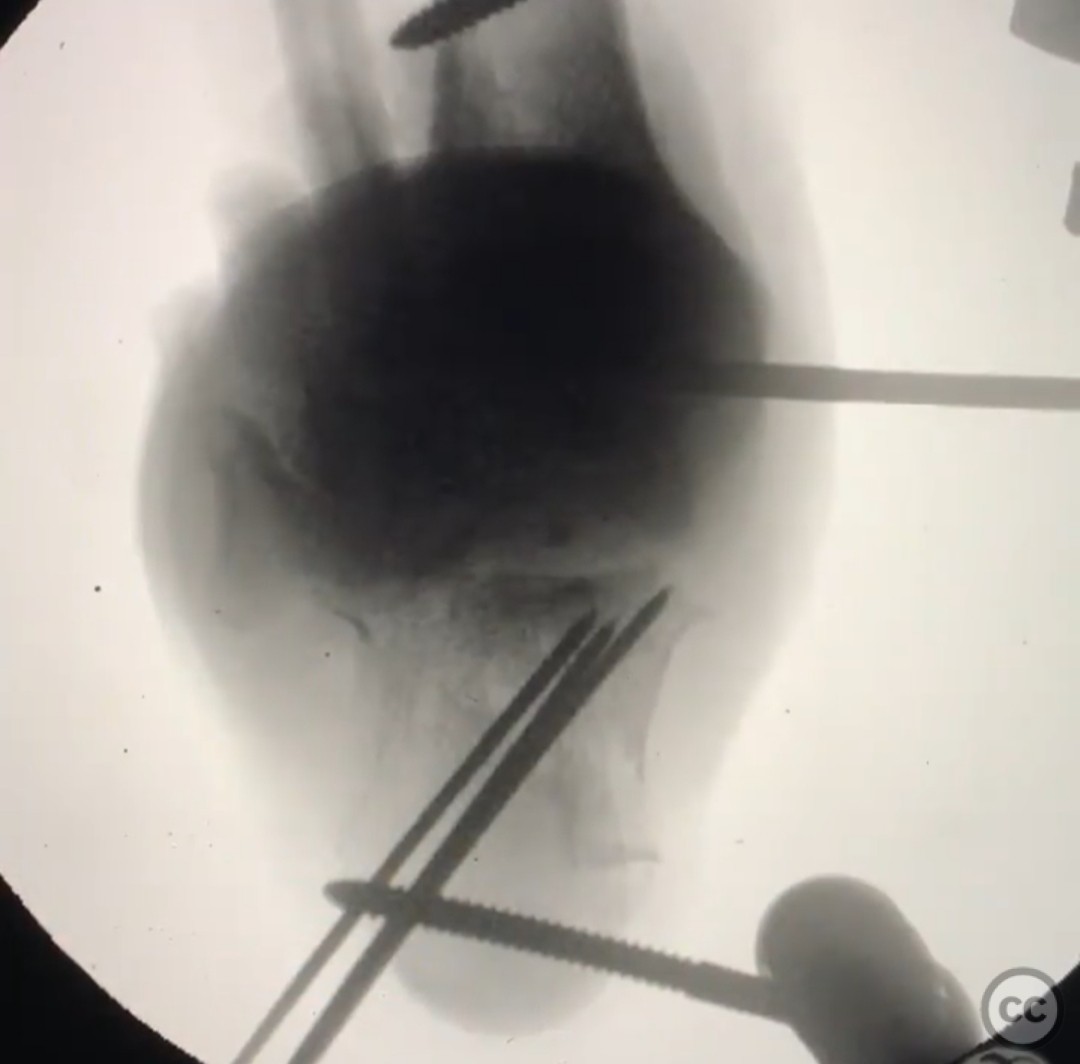
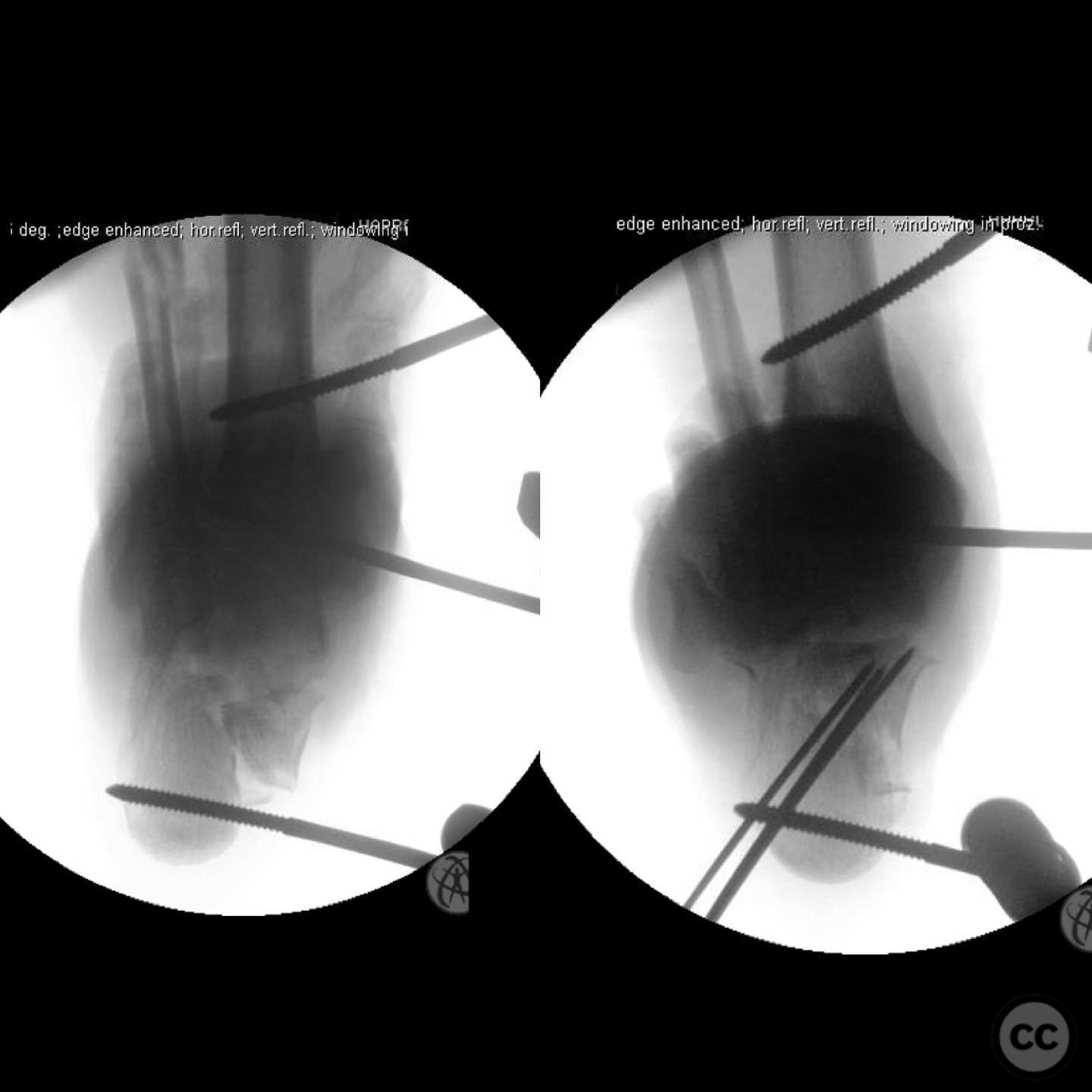
Anatomical surgical approach: A percutaneous approach was utilized for the reduction of the posterior facet. A wire was used for localization, followed by a small incision to allow for manipulation of the facet using blunt instruments. The reduction was secured with wiring, avoiding penetration through lateral skin structures.
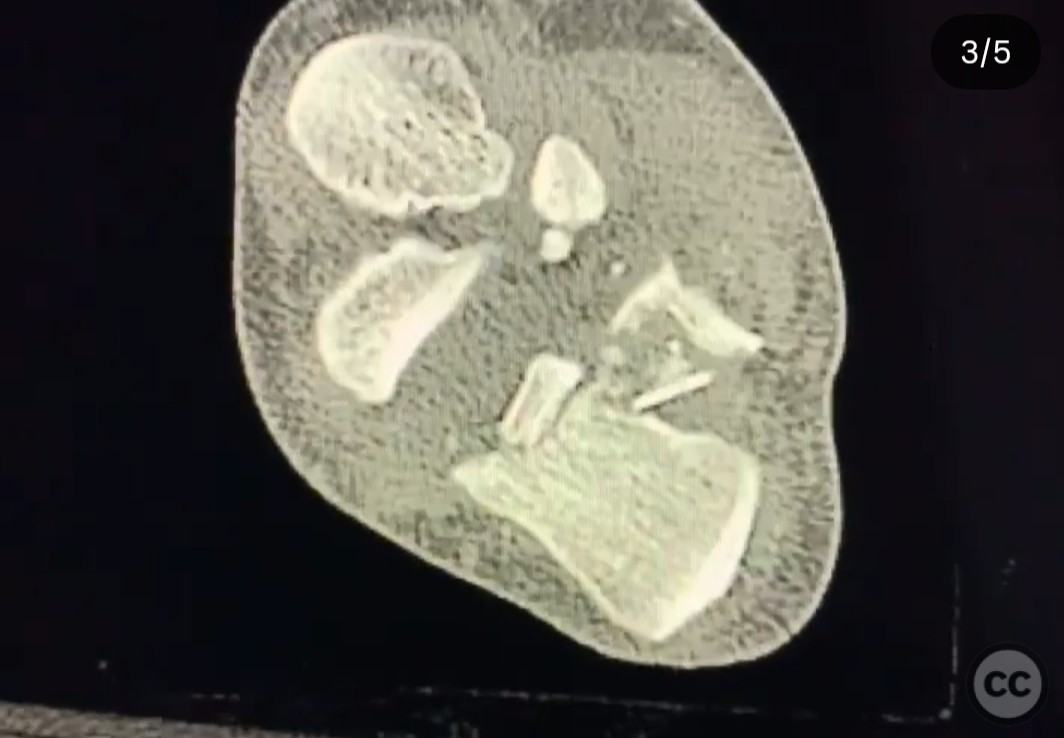
Operative remarks:The surgeon emphasized the urgency of reducing the posterior facet to prevent skin necrosis and potential amputation. The use of a medial external fixator was crucial in creating space for reduction by distracting and elevating the talus. Post-reduction CT confirmed improved alignment, although further interventions were anticipated.
Postoperative protocol: Initial immobilization with a medial external fixator, followed by gradual weight-bearing as tolerated. Close monitoring of skin integrity and neurovascular status was advised.
Follow up: Not specified.
Orthopaedic implants used: Medial external fixator, percutaneous wires for reduction stabilization.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 291 times
21 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Complete Posterior Facet Dislocation of the Calcaneus with Medial Wall Displacement.. Journal of Orthopaedic Surgery and Traumatology. Case Report 21965399 Published Online Jul 21 2025.