














Polytrauma with Peri-implant Humerus Fracture Management
Score and Comment on this Case
Clinical Details
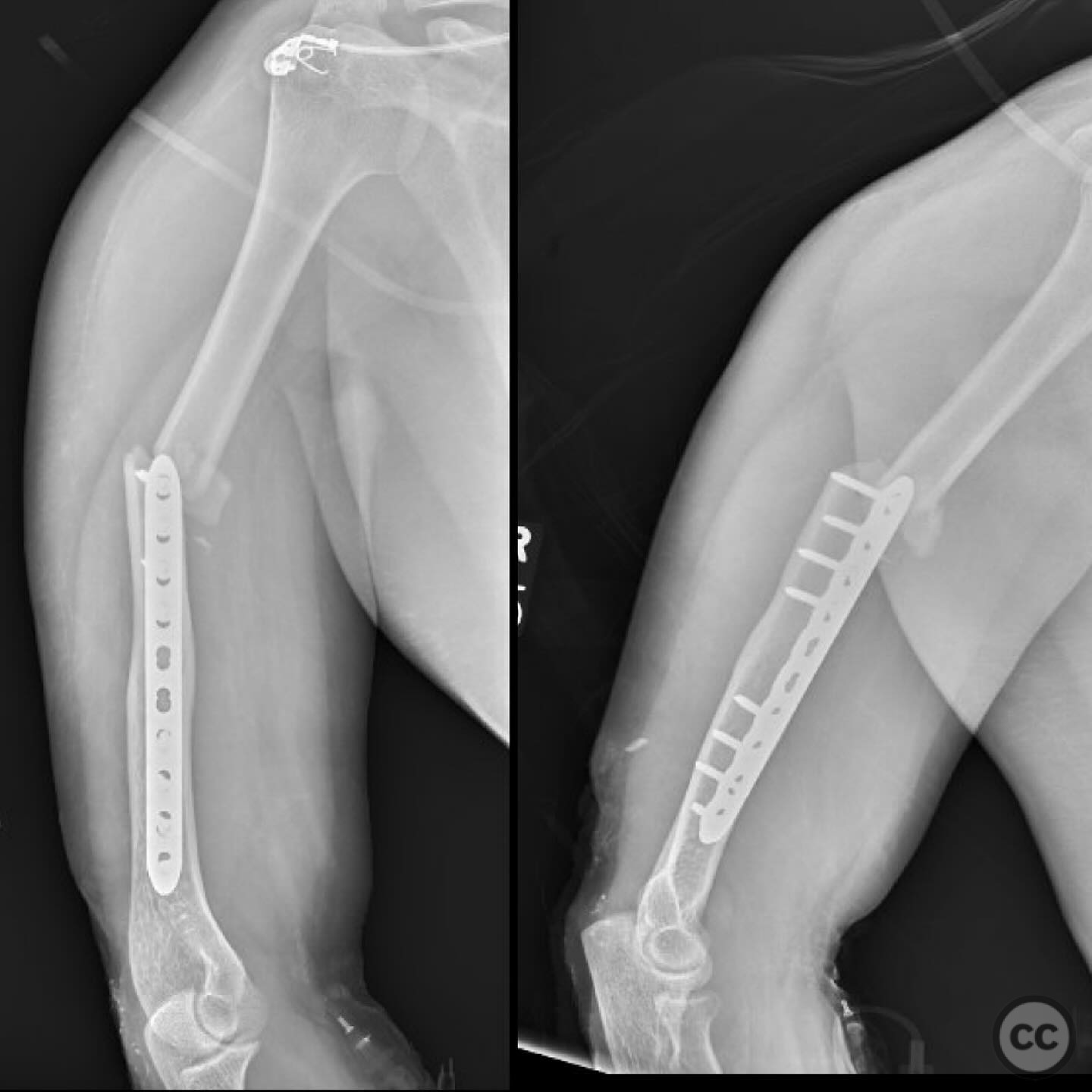
Clinical and radiological findings: A 33-year-old male involved in a motor vehicle collision presented with multiple injuries: a closed femur fracture, a closed peri-implant humerus fracture, and a type 2 open proximal ulna fracture with some associated ligamentous injury or instability. Initial lactate level was 5.5 mmol/L in the emergency department, which decreased to 3.5 mmol/L following appropriate resuscitation. The patient was hemodynamically stable on one vasopressor, with no major head, chest, or abdominal injuries.
Preoperative Plan
Planning remarks: The surgical plan for the humerus involved a posterior modified modified Gerwin approach (lateral paratricepital approach), avoiding the anterolateral plate altogether. This approach was chosen due to its favorable anatomical exposure and ability to access the entire length of the humerus.
Surgical Discussion
Patient positioning: The patient was positioned prone on the operating table to facilitate the posterior approach to the humerus.
Anatomical surgical approach: A posterior modified modified Gerwin approach was utilized, involving a lateral paratricepital incision. The dissection proceeded between the heads of the triceps brachii muscle, with proximal dissection under the deltoid muscle, providing access to the humeral shaft while avoiding interference with the existing anterolateral plate.
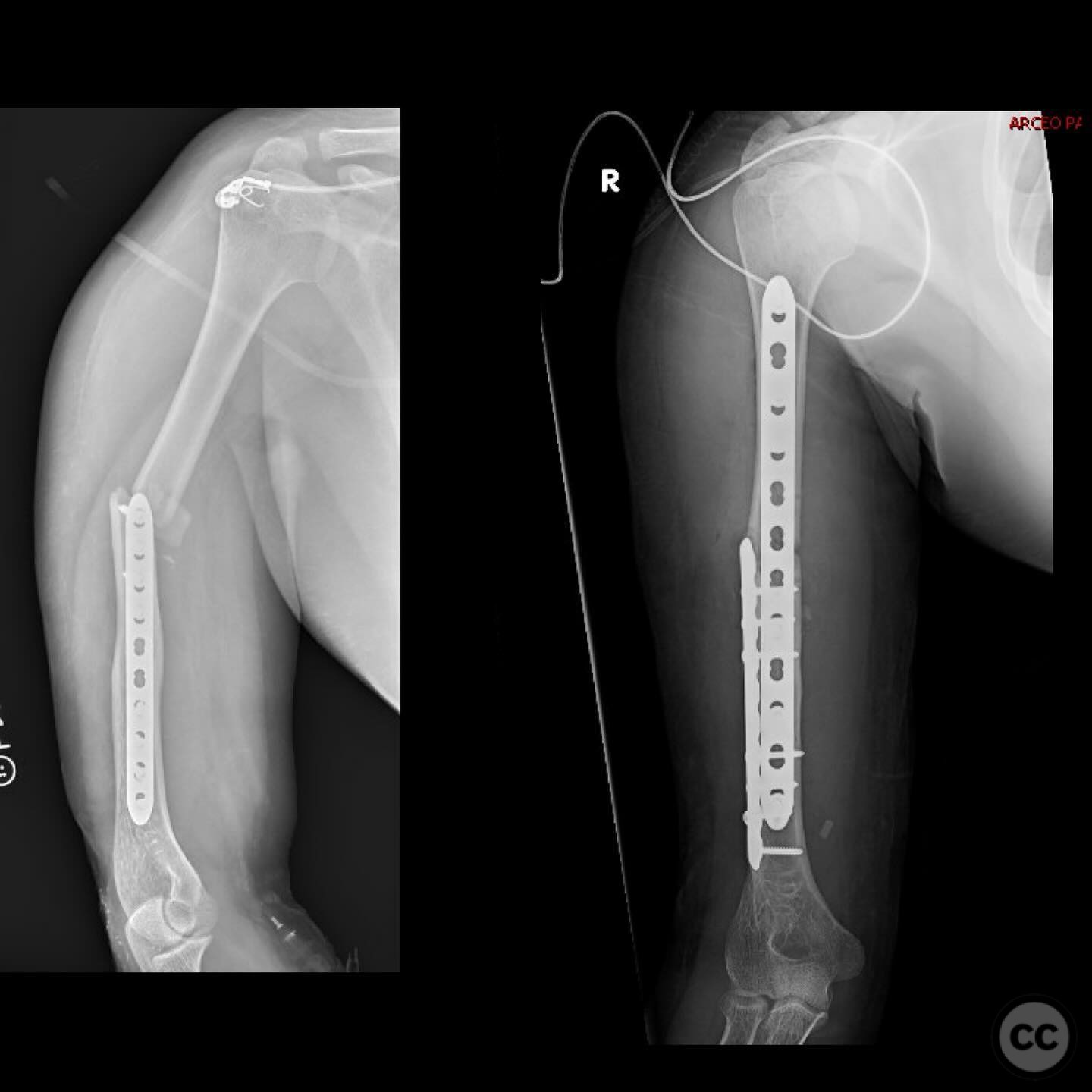
Operative remarks:The humerus fracture was reduced using straight modified Weber clamps and stabilized with a preloaded 4.5 mm narrow LCDC plate in compression mode. The reduction was rated as 4.5/5 on the anteroposterior view but only 3/5 on the lateral view due to a slight apex anterior malreduction. This malreduction was attributed to the lack of far cortex support and insufficient pre-bending of the plate prior to compression.
Postoperative protocol: Postoperative rehabilitation included early mobilization with weight-bearing as tolerated for the lower extremity fractures and protected range of motion exercises for the upper extremity.
Follow up: Not specified
Orthopaedic implants used: Preloaded 4.5 mm narrow LCDC plate
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 346 times
10 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Polytrauma with Peri-implant Humerus Fracture Management. Journal of Orthopaedic Surgery and Traumatology. Case Report 20942148 Published Online Jul 10 2025.