












Distal Tibial Shaft Nonunion with Valgus and Rotational Deformity
Score and Comment on this Case
Clinical Details
Clinical and radiological findings: A 33-year-old male mechanic and motocross enthusiast presented with an inability to walk more than a few blocks without significant pain, worsening over time. The patient had sustained a closed distal third tibial fracture with an associated proximal fibula fracture 9 months prior, treated elsewhere. There was no history of infection, and the patient had no other medical problems. He was a smoker, consuming half to a full pack of cigarettes daily, but had quit smoking by the time of presentation. Radiological assessment revealed an aseptic oligo/hypertrophic nonunion with 18 degrees of valgus and 30 degrees of external rotational deformities. The proximal fibula fracture was also in nonunion. Laboratory tests for nonunion were normal.
Preoperative Plan
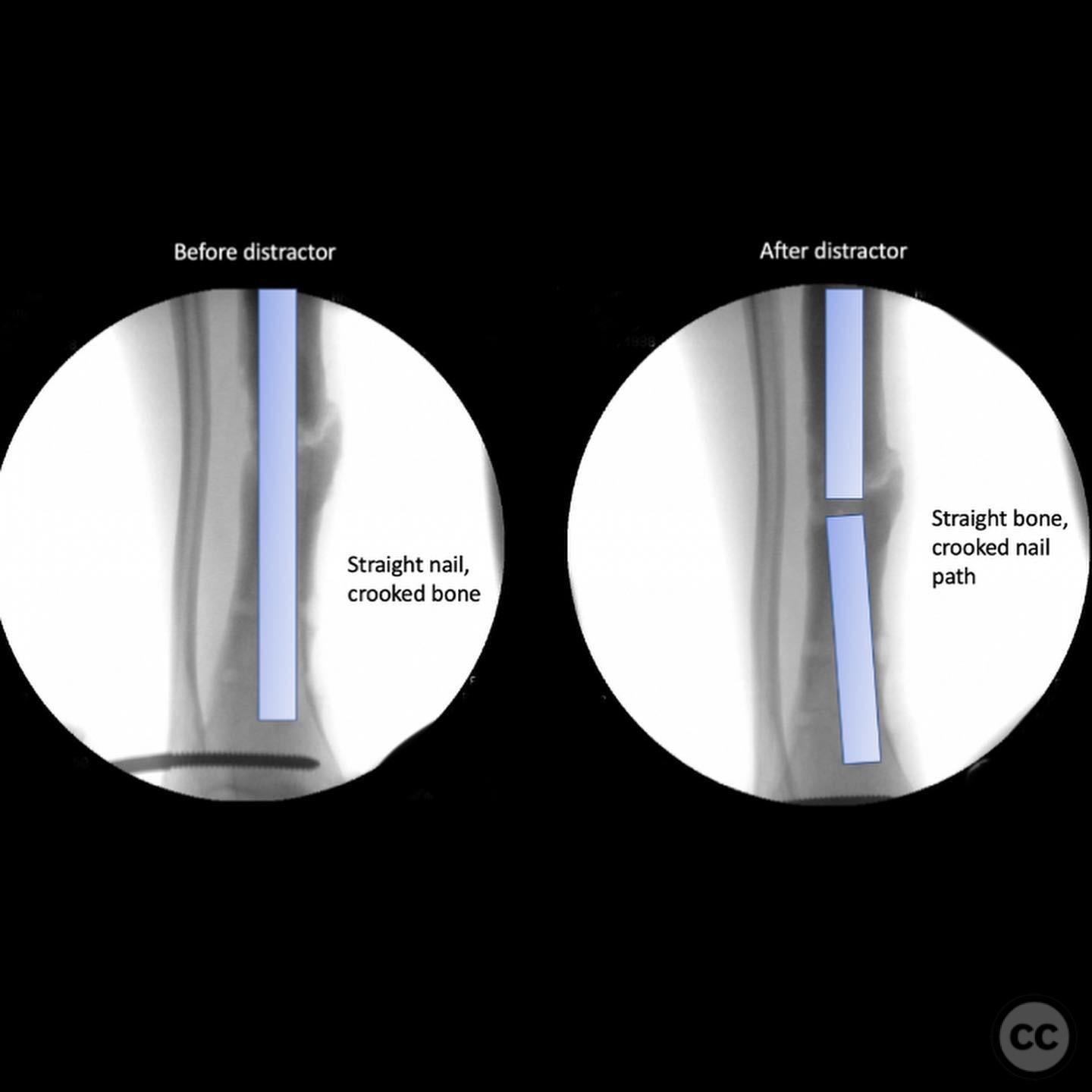
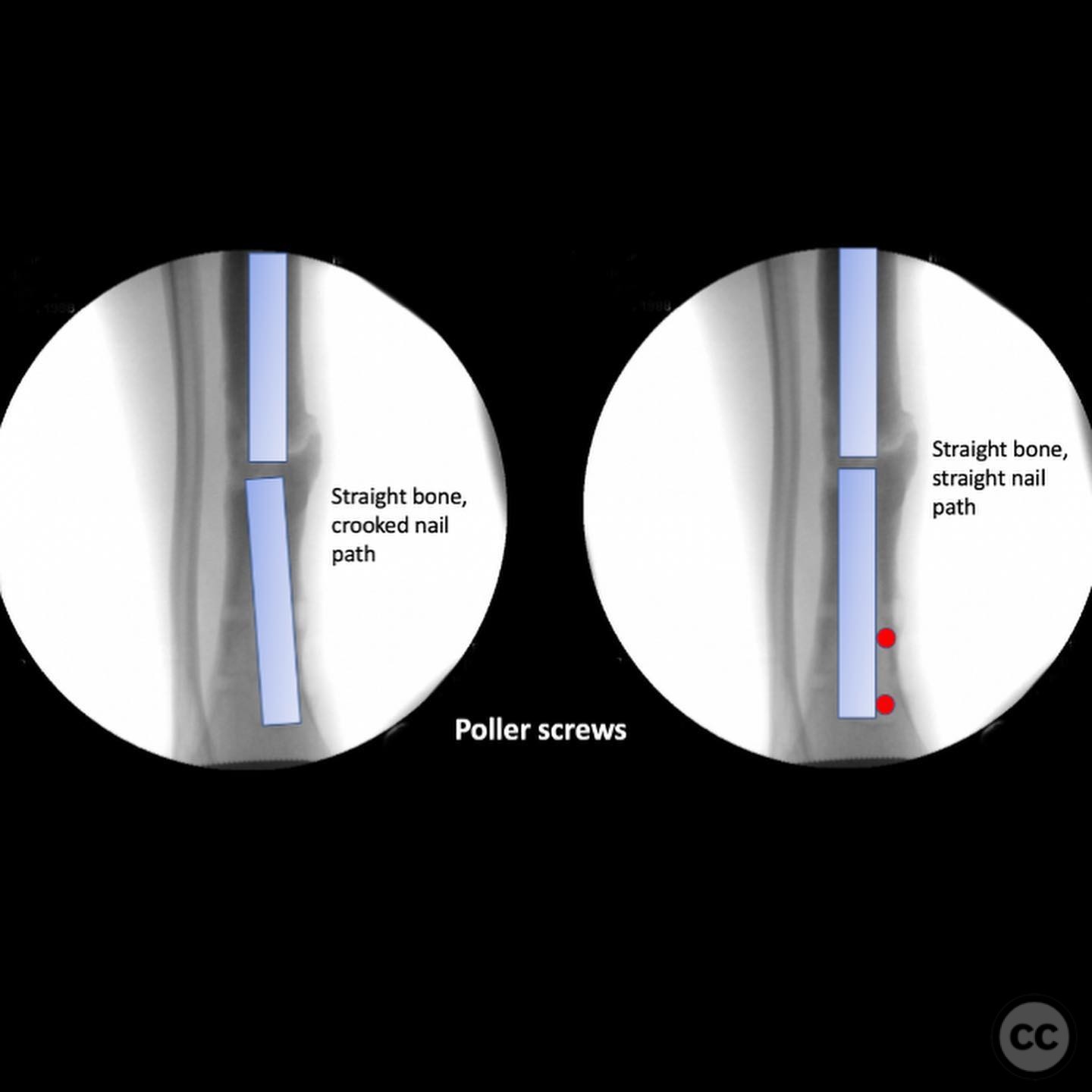
Planning remarks: The preoperative plan involved indirect techniques to restore length, alignment, and rotation of the tibia. A laterally based distractor was planned to be placed with pins parallel to the joint surfaces to apply a varus force and internal rotation correction. Poller screws were planned to redirect reamers and the intramedullary nail to achieve proper alignment.
Surgical Discussion
Patient positioning: The patient was positioned supine on the operating table with the affected leg prepared for lateral distractor placement.
Anatomical surgical approach: A lateral approach was utilized for the placement of the distractor. Pins were inserted parallel to the joint surfaces to facilitate manipulation of the tibial alignment. Poller screws were placed percutaneously to guide the reaming process and nail insertion.
Operative remarks:The surgeon applied a massive varus force combined with 30 degrees of internal rotation using the distractor to correct the deformity. Intraoperative fluoroscopy confirmed the correction. Poller screws were employed to redirect the reamers and nail, ensuring proper alignment and preventing recurrence of the deformity. An 11mm intramedullary nail was inserted, as larger diameters could not be accommodated past the blocking screws.
Postoperative protocol: Postoperatively, weight-bearing was restricted initially, with gradual progression based on radiographic evidence of union and clinical symptoms. Physical therapy focused on range of motion and strengthening exercises.
Follow up: Not specified
Orthopaedic implants used: Intramedullary nail, Poller screws, Lateral distractor
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 322 times
13 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Distal Tibial Shaft Nonunion with Valgus and Rotational Deformity. Journal of Orthopaedic Surgery and Traumatology. Case Report 20806490 Published Online Jul 13 2025.