


Complex Distal Tibial Fracture with Soft Tissue Compromise and Medial Malleolar Avulsion.
Score and Comment on this Case
Clinical Details
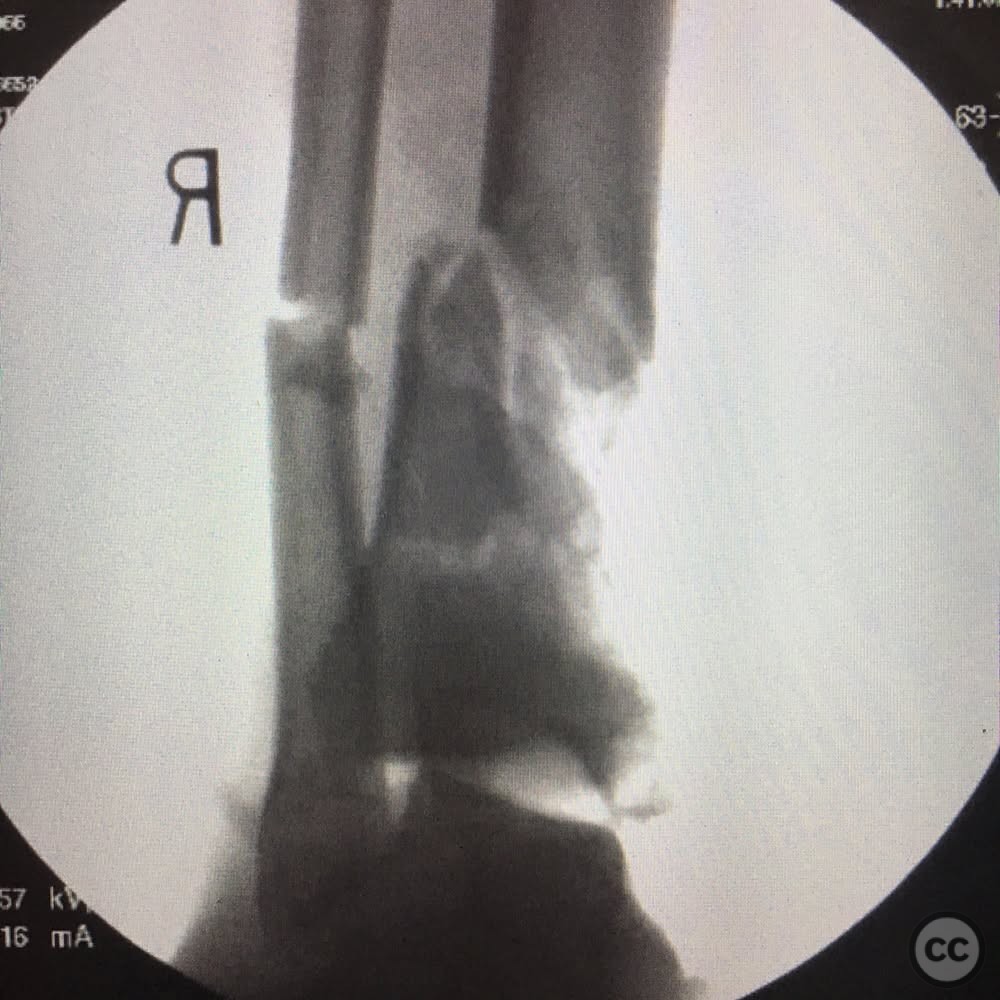
Clinical and radiological findings: A middle-aged male roofer sustained a high-energy motorcycle accident resulting in a Gustilo-Anderson type IIIB open fracture of the distal tibia. The injury presented with significant soft tissue damage, including laceration of the posterior tibial artery, which was compensated by anterior tibial artery and collateral circulation, maintaining foot perfusion. The tibial nerve was intact with some neuropraxia noted. Posterior tibialis, flexor digitorum longus (FDL), and flexor hallucis longus (FHL) tendons were lacerated. Radiographs and intraoperative fluoroscopy revealed significant metaphyseal comminution, an unstable tibiotalar joint, and a complete deltoid ligament avulsion with an associated avulsed posterior colliculus of the medial malleolus.
Preoperative Plan
Planning remarks: The preoperative plan involved initial stabilization of the ankle joint to restore tibial length, followed by soft tissue repair. The posterior tibialis tendon and FHL were directly repaired, while the FDL was tenodesed to the FHL. The medial malleolar fracture with deltoid ligament avulsion was addressed using a 2.0 mm screw and Fiberwire through a bone tunnel. A fibular nail was used for length stability, and an ankle-spanning external fixator was applied for temporary stabilization.
Surgical Discussion
Patient positioning: The patient was positioned supine on the operating table with the affected limb prepped and draped in standard sterile fashion.
Anatomical surgical approach: A medial approach to the distal tibia was utilized for fracture fixation. The incision allowed access to the medial malleolus for fixation of the avulsed fragment and deltoid ligament repair. The fibula was accessed laterally for intramedullary nailing. An external fixator was applied spanning the ankle joint to maintain reduction and stability.
Operative remarks:The surgeon noted that despite the complexity of the injury and the initial concerns regarding the potential for implant failure, the chosen method of fixation proved successful. The medial bridge plate provided adequate stability until union, despite initial doubts about its sufficiency given the large bone defect. The use of antibiotic-impregnated cement to fill the bone void and subsequent autogenous bone grafting contributed to successful healing without infection or implant failure.
Postoperative protocol: Postoperatively, the patient was non-weight bearing on the affected limb for six weeks. Progressive weight bearing was initiated following confirmation of graft incorporation and satisfactory healing progress.
Follow up: Not specified.
Orthopaedic implants used: 2.0 mm screw, Fiberwire, fibular intramedullary nail, ankle-spanning external fixator, medial bridge plate, antibiotic-impregnated cement.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 386 times
28 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Complex Distal Tibial Fracture with Soft Tissue Compromise and Medial Malleolar Avulsion.. Journal of Orthopaedic Surgery and Traumatology. Case Report 20016278 Published Online Jul 28 2025.