


Percutaneous Iliosacral and Anterior Iliac Screw Fixation for AO/OTA 61-B2 Pelvic Ring Injury
Score and Comment on this Case
Clinical Details
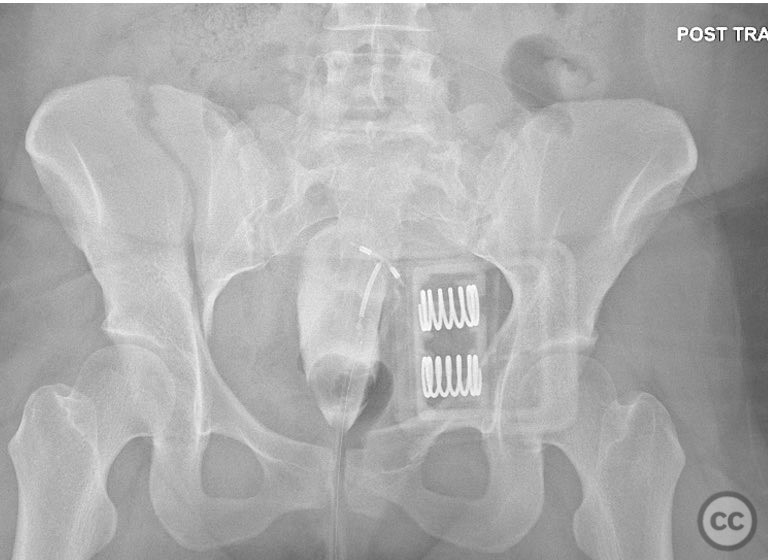
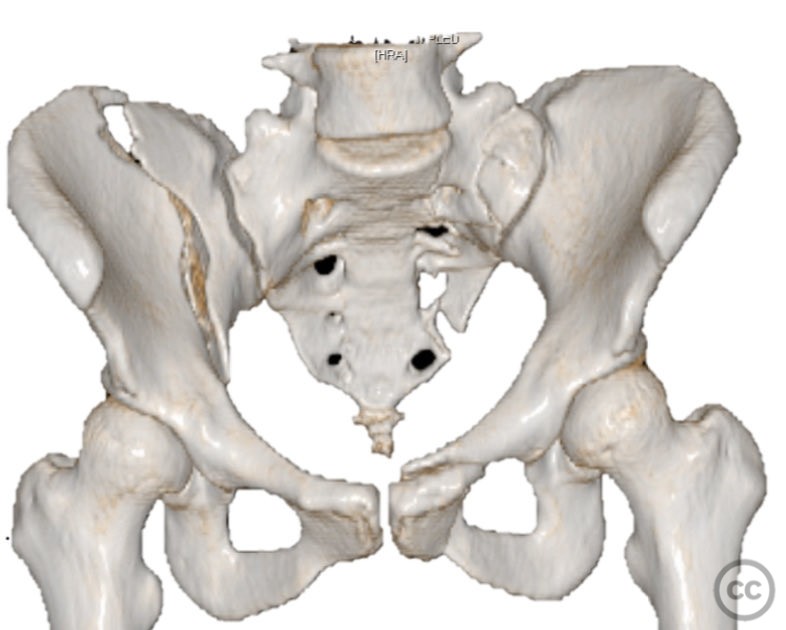
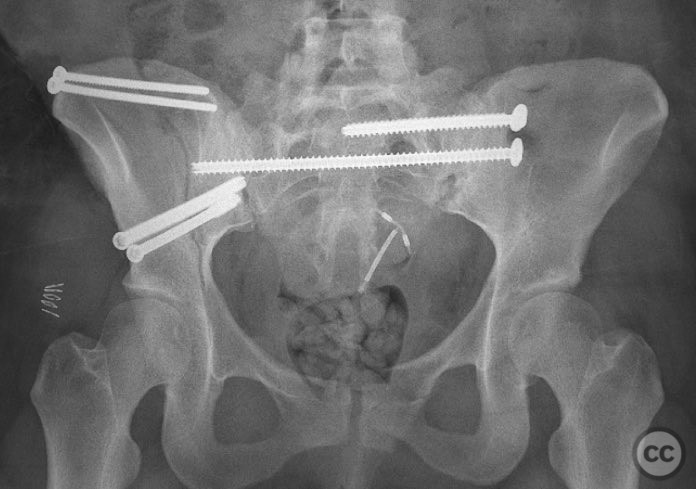
Clinical and radiological findings: A 26-year-old female sustained a closed pelvic ring injury following a motor vehicle accident. She was hemodynamically stable, neurologically intact, and had no other associated injuries. Skin integrity was preserved. Initial management included pelvic binder application and 10 pounds of distal femoral skeletal traction. Portable AP pelvic radiograph demonstrated a left-sided sacral fracture with associated ipsilateral iliac wing and pubic ramus fractures, consistent with an AO/OTA 61-B2 (lateral compression type II) injury pattern.
Preoperative Plan
Planning remarks: The preoperative plan included supine positioning with maintenance of skeletal traction. The left sacral fracture was to be stabilized first with percutaneous iliosacral screw fixation. An anterior iliac approach was planned for direct reduction and fixation of the iliac wing fracture, followed by medullary screw fixation of the iliac crest and pelvic brim. Intraoperative fluoroscopic stress testing of the left pubic ramus fracture and overall pelvic ring stability was planned.
Surgical Discussion
Patient positioning: The patient was positioned supine on the operating table with a bump placed beneath the pelvis to facilitate reduction, while maintaining distal femoral skeletal traction.
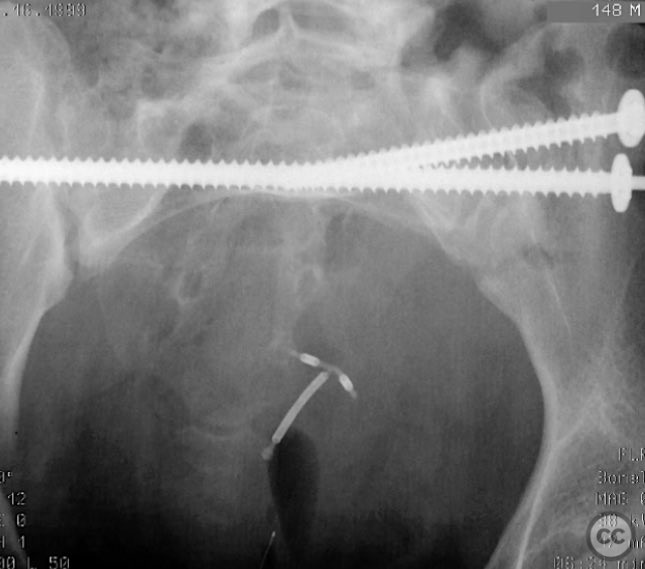
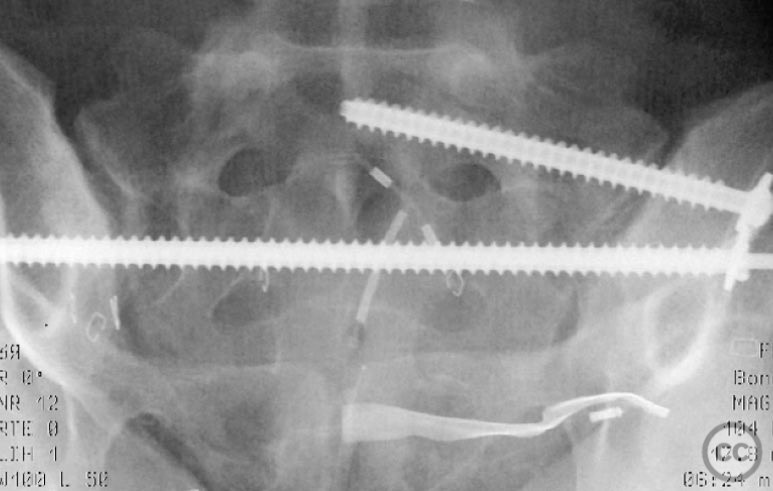
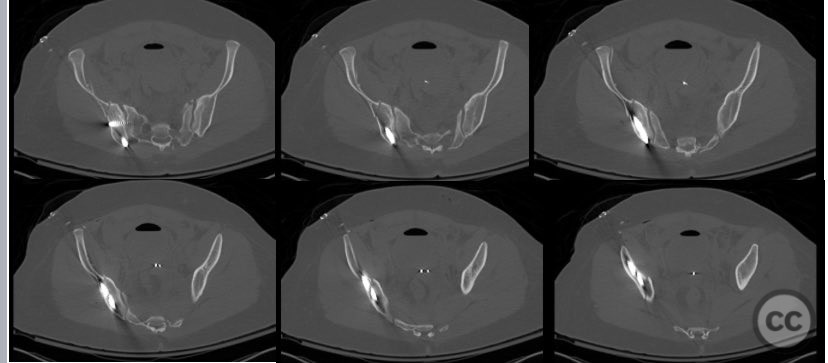
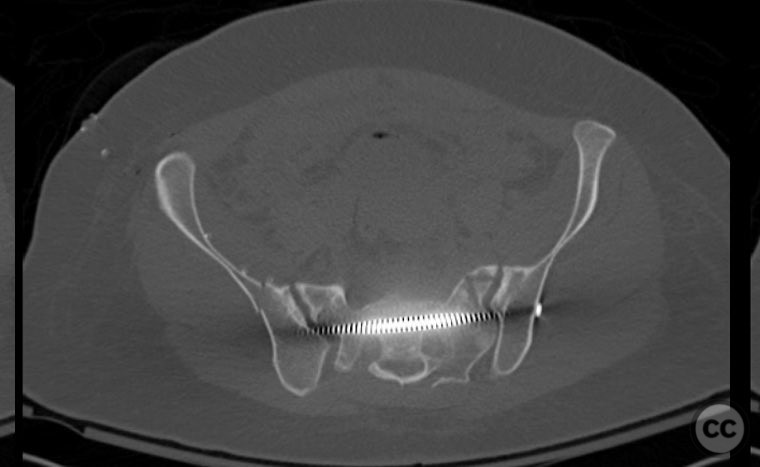
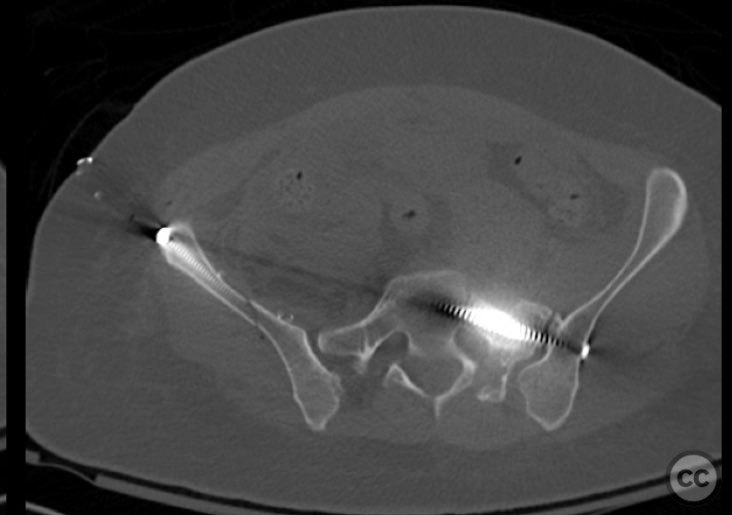
Anatomical surgical approach: The left sacral fracture was addressed first via percutaneous placement of iliosacral screws under fluoroscopic guidance. An anterior approach to the iliac wing was performed via a longitudinal incision along the crista iliaca, subperiosteal dissection to expose the fractura alae ossis ilii, followed by debridement, reduction, and temporary clamping. Definitive fixation was achieved with two 7mm diameter cannulated fully threaded medullary screws placed across the iliac crest and pelvic brim into the corpus ossis ilii. The left ramus ossis pubis fracture and overall cingulum pelvicum were assessed intraoperatively with fluoroscopy for residual instability.
Operative remarks:Intraoperatively, minimal residual deformity of the left hemipelvis was noted after traction and positioning. The sacral fracture was stabilized first with iliosacral screws. The anterior iliac exposure allowed for direct visualization, cleaning, reduction, and clamping of the iliac wing fracture prior to screw fixation. After fixation, intraoperative fluoroscopic stress examination demonstrated stability of the left pubic ramus fracture and overall pelvic ring, obviating the need for further anterior fixation.
Postoperative protocol: The patient was restricted to bed-to-chair transfers and non-weightbearing activity for the first five weeks postoperatively.
Follow up: Not specified
Orthopaedic implants used: Two 7mm diameter cannulated fully threaded medullary screws (iliac crest and pelvic brim), percutaneous iliosacral screw(s).
Search for Related Literature


Industry Sponsership
contact us for advertising opportunities
Article viewed 668 times
12 Sep 2025
Add to Bookmarks
Full Citation
Cite this article:
Routt, ML. (2025). Percutaneous Iliosacral and Anterior Iliac Screw Fixation for AO/OTA 61-B2 Pelvic Ring Injury. Journal of Orthopaedic Surgery and Traumatology. Case Report 19615561 Published Online Sep 12 2025.