
Comminuted Subcapital Femoral Neck Fracture Treated via Heuter Approach
Score and Comment on this Case
Clinical Details
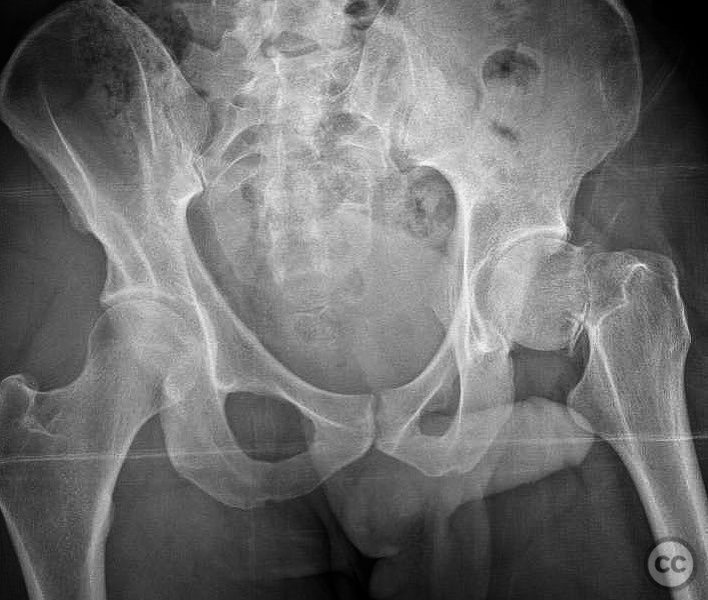
Clinical and radiological findings: A 34-year-old male sustained a fall from a height of 5 feet directly onto his left hip while at work. Initial clinical examination suggested a significant injury to the hip, and subsequent axial CT imaging confirmed a comminuted subcapital femoral neck fracture, particularly involving the inferior calcar region. The fracture was classified as AO/OTA 31-B2.
Preoperative Plan
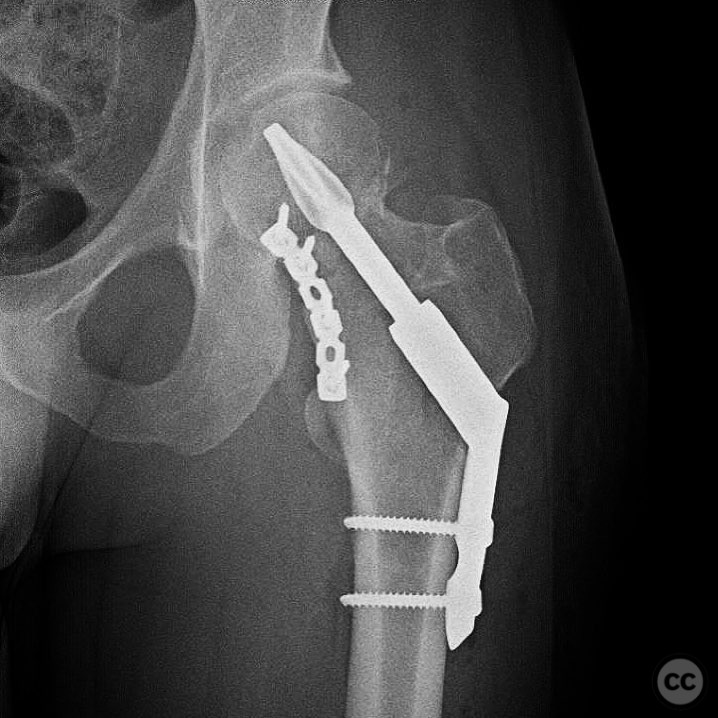
Planning remarks: The preoperative plan involved a direct reduction of the fracture through a Heuter approach. The strategy included the use of a 2.5mm Schanz pin for manipulative reduction and a straight modified Weber clamp to obtain and maintain reduction. Due to calcar comminution, an anterior inferior 2.7mm reconstruction plate was planned to maintain reduction during definitive implant insertion.
Surgical Discussion
Patient positioning: Supine positioning on a radiolucent table to facilitate intraoperative imaging and access.
Anatomical surgical approach: A direct anterior Heuter approach was utilized, involving an incision over the anterior aspect of the hip. Dissection proceeded through the interval between the sartorius and tensor fascia lata muscles, providing access to the hip joint capsule. Capsulotomy was performed to expose the femoral neck and head for reduction.
Operative remarks:The surgeon noted the utility of a 2.5mm Schanz pin in the femoral head for manipulative reduction, combined with a straight modified Weber clamp for maintaining reduction. The anterior inferior 2.7mm reconstruction plate served as a buttress against varus collapse and functioned similarly to an anti-rotation screw, providing robust support during definitive fixation with a fixed angle device. The surgeon emphasized the importance of achieving an anatomic reduction over the timing of surgery for optimal outcomes.
Postoperative protocol: Postoperative rehabilitation included early mobilization with toe-touch weight bearing (TTWB) for 6 weeks, followed by progressive weight bearing as tolerated. Range of motion exercises were initiated immediately post-surgery to prevent stiffness.
Follow up: Not specified.
Orthopaedic implants used: 2.5mm Schanz pin, 2.7mm reconstruction plate, fixed angle device.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 387 times
04 Aug 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Comminuted Subcapital Femoral Neck Fracture Treated via Heuter Approach. Journal of Orthopaedic Surgery and Traumatology. Case Report 18031620 Published Online Aug 04 2025.