


High-Energy Trauma Case: Managing Combined Pelvic Ring and Acetabular Fractures with Proximal Femur Displacement
Score and Comment on this Case
Clinical Details
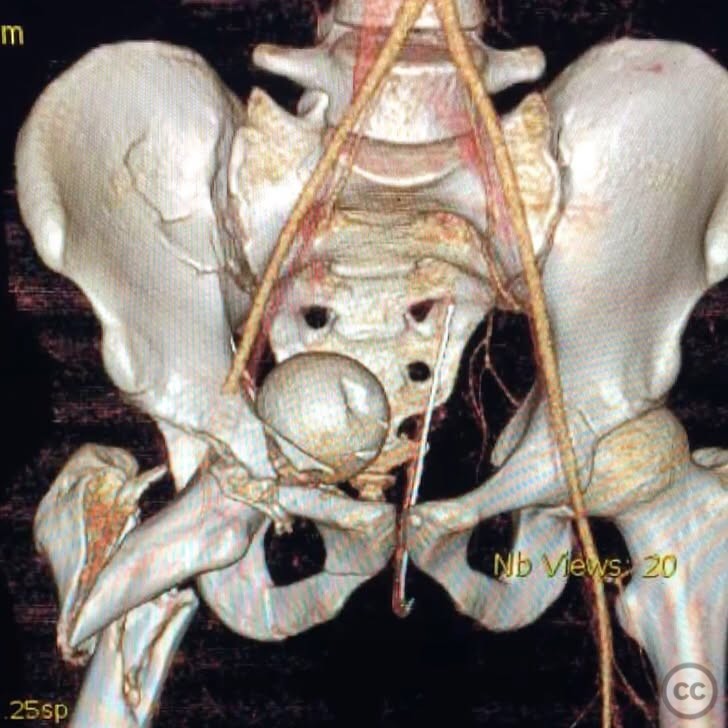
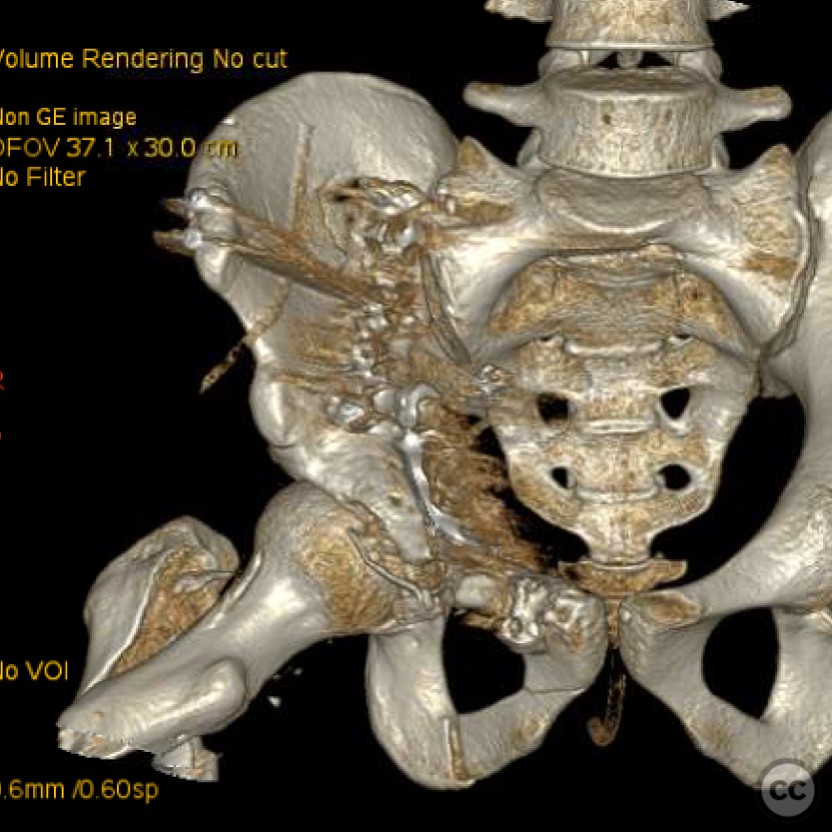
Clinical and radiological findings: A 29-year-old patient was ejected from a vehicle at high speed, resulting in a complex pelvic ring and acetabular fracture with proximal femur displacement. Initial CT 3D reconstruction revealed significant disruption of the pelvic ring and acetabulum, with the proximal femur displaced into the pelvis. The injury was closed with no neurovascular compromise noted. The proximal femur could not be reduced with traction alone, necessitating a brim osteotomy and distraction for reduction.
Preoperative Plan
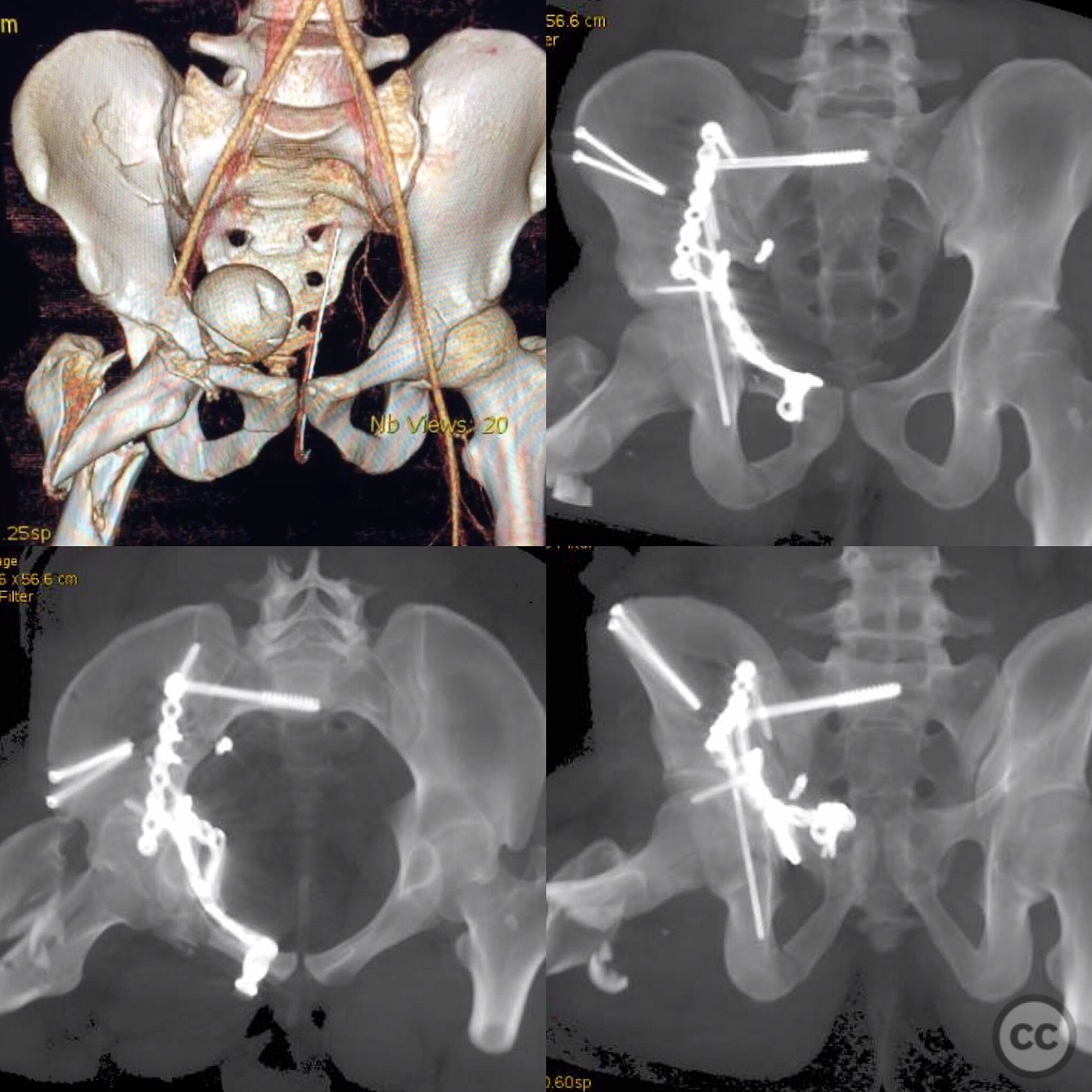
Planning remarks: The preoperative plan involved addressing the pelvic ring and acetabular fractures. The surgical sequence began with stabilization of the sacroiliac joint to restore pelvic ring integrity, followed by acetabular reconstruction. For the acetabulum, an ilioinguinal approach was planned to allow direct access for reduction and fixation. The proximal femur required a Watson-Jones approach for open reduction and fixation.
Surgical Discussion
Patient positioning: The patient was positioned laterally to facilitate access to both the acetabulum and proximal femur. This positioning allowed for easier manipulation and reduction of the displaced fragments.
Anatomical surgical approach: A Watson-Jones approach was utilized for the proximal femur, involving an incision over the lateral aspect of the hip, followed by dissection through the interval between the tensor fasciae latae and gluteus medius. Subperiosteal elevation was performed to expose the femoral head and neck for reduction.
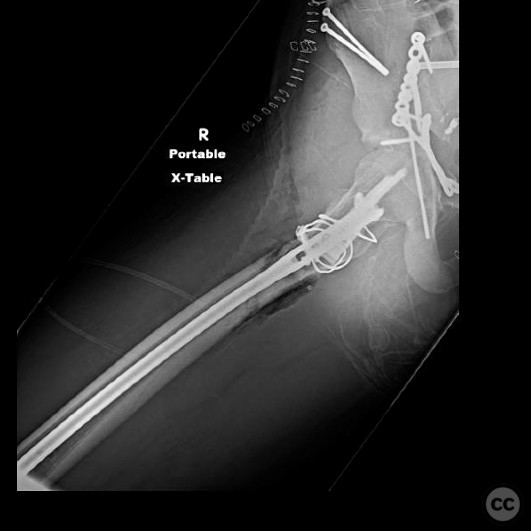
Operative remarks:The surgeon noted that closed reduction on a fracture table was not feasible due to the deforming forces on the fracture fragments. Open reduction was achieved using a GT hook plate for stabilization of the greater trochanter, followed by insertion of an antegrade reamed reconstruction nail starting at the "trochiformis" region. The choice of implants was critical to avoid high failure rates associated with proximal femoral locked plating or blade plates.
Postoperative protocol: Postoperative rehabilitation included protected weight-bearing with crutches for 6 weeks, followed by gradual progression to full weight-bearing as tolerated. Range of motion exercises were initiated early to prevent joint stiffness.
Follow up: Not specified.
Orthopaedic implants used: GT hook plate, antegrade reamed reconstruction nail.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 285 times
26 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). High-Energy Trauma Case: Managing Combined Pelvic Ring and Acetabular Fractures with Proximal Femur Displacement. Journal of Orthopaedic Surgery and Traumatology. Case Report 17831922 Published Online Jul 26 2025.