



Complete Iliac Fracture with Symphysis Pubis Disruption and Contralateral Incomplete SI/Iliac Fracture
Score and Comment on this Case
Clinical Details
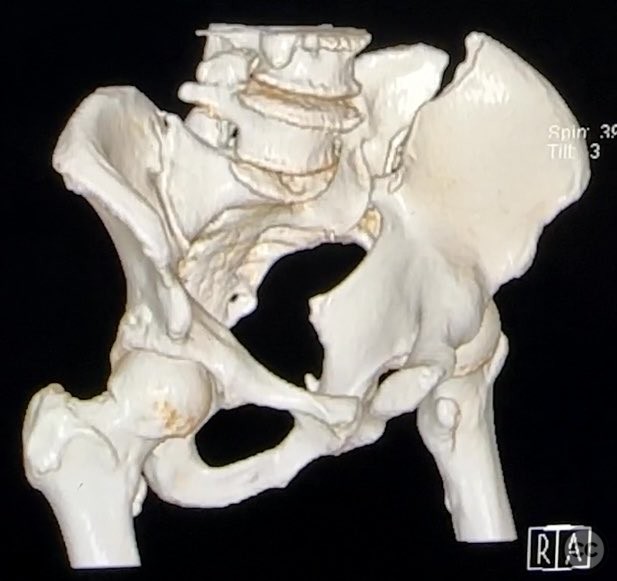
Clinical and radiological findings: A patient sustained a high-energy pelvic ring injury characterized by a complete left iliac fracture extending from the iliac crest to the greater sciatic notch, associated with a complete disruption of the symphysis pubis (SP). Additionally, there was a less displaced, incomplete right sacroiliac (SI)/iliac fracture. The injury pattern is consistent with an AO/OTA 61-B2.3 (lateral compression type II) pelvic ring injury. No neurovascular compromise or significant soft tissue injury was reported.
Preoperative Plan
Planning remarks: The preoperative plan included open reduction and internal fixation of both the iliac fracture and the symphysis pubis disruption. The anatomical approach was planned via direct anterior exposure to the symphysis pubis and an ilioinguinal approach to the iliac wing fracture, with reduction maneuvers at both the iliac crest and pelvic brim.
Surgical Discussion
Patient positioning: The patient was positioned supine with a sacral bump to facilitate reduction, and left-sided longitudinal traction was applied to aid in fracture alignment.
Anatomical surgical approach: The surgical approach involved a direct anterior midline exposure to the symphysis pubis, followed by subperiosteal dissection to expose the disrupted SP. The ilioinguinal approach was utilized for the iliac fracture, with careful elevation of the abdominal musculature from the iliac crest and pelvic brim. The iliac fracture was reduced using a Farabeuf clamp at the linea terminalis (brim) and a tenaculum at the crista iliaca. The symphysis pubis was reduced with a tenaculum clamp.
Operative remarks:Accurate anatomical reduction was achieved at both the iliac crest and pelvic brim using direct clamp application. Stable fixation was performed at each site according to biomechanical principles, utilizing plates and/or screws as indicated by fragment size and displacement. For closure of the symphysis pubis, interrupted 2-0 Vicryl pop-off sutures on a non-cutting needle were used for the midline portion, with additional 0 Vicryl sutures for reinforcement at the tendon insertion area.
Postoperative protocol: Postoperative rehabilitation protocol included initial bed rest with protected weight bearing, progressing to partial weight bearing as tolerated by 6 weeks, and full weight bearing by 10–12 weeks postoperatively, depending on radiographic evidence of healing and clinical stability.
Follow up: Not specified
Orthopaedic implants used: Pelvic reconstruction plate(s), cortical screws, 2-0 Vicryl sutures, 0 Vicryl sutures
Search for Related Literature


Industry Sponsership
contact us for advertising opportunities
Article viewed 301 times
12 Sep 2025
Add to Bookmarks
Full Citation
Cite this article:
Routt, ML. (2025). Complete Iliac Fracture with Symphysis Pubis Disruption and Contralateral Incomplete SI/Iliac Fracture. Journal of Orthopaedic Surgery and Traumatology. Case Report 17775518 Published Online Sep 12 2025.