







Complex Essex-Lopresti Variant: Comminuted Radial Head Fracture Managed with ORIF and LUCL Reconstruction
Score and Comment on this Case
Clinical Details
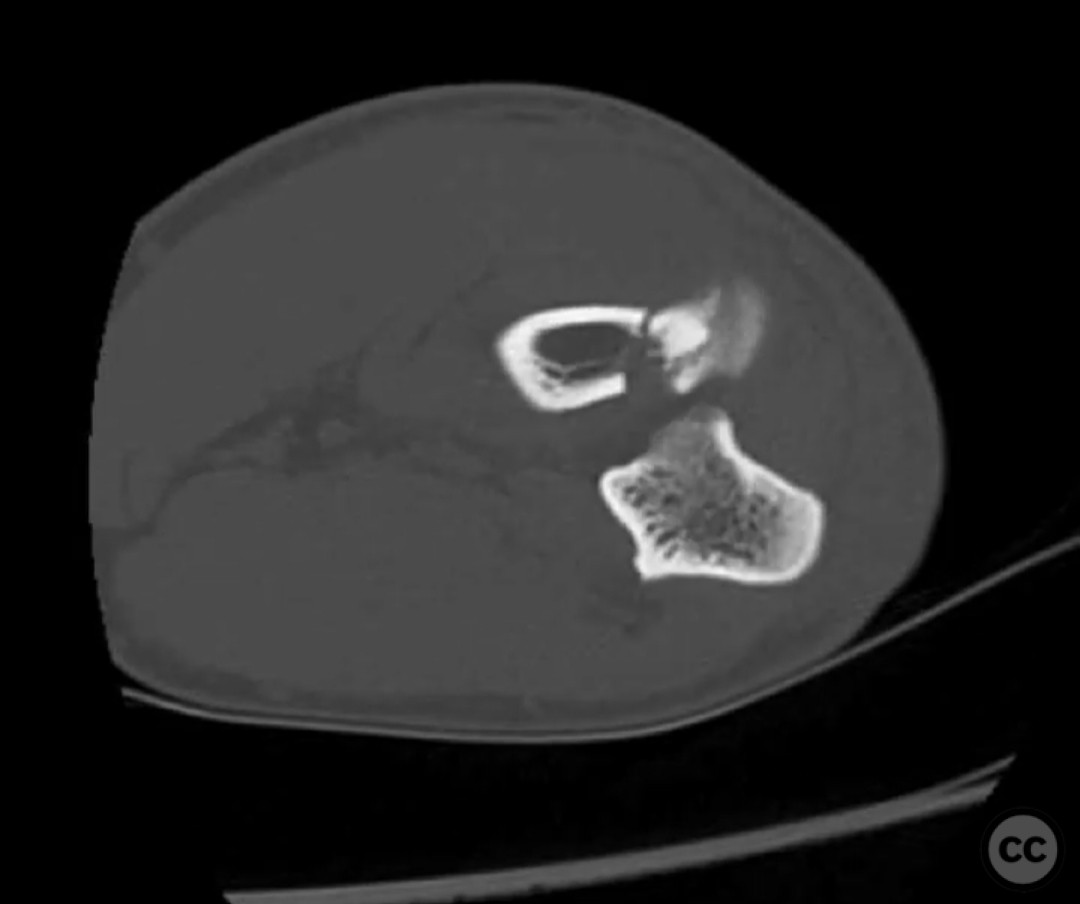
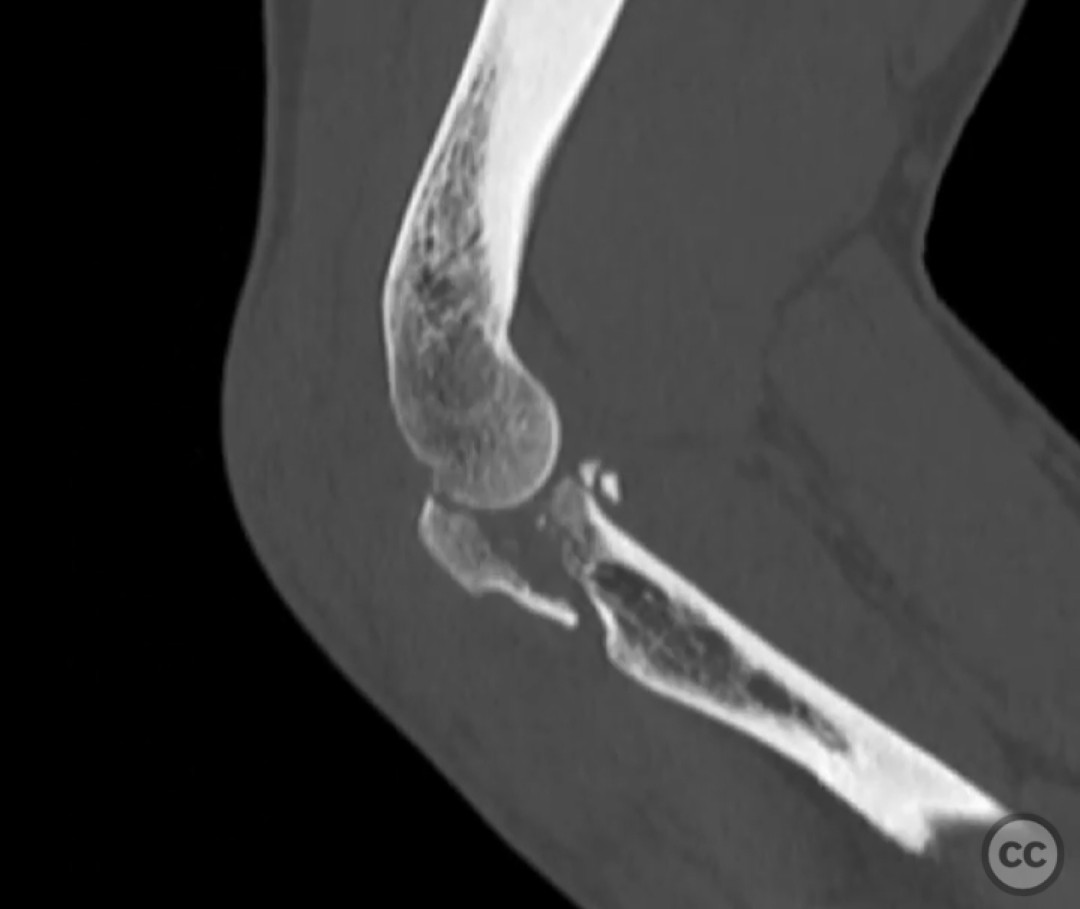
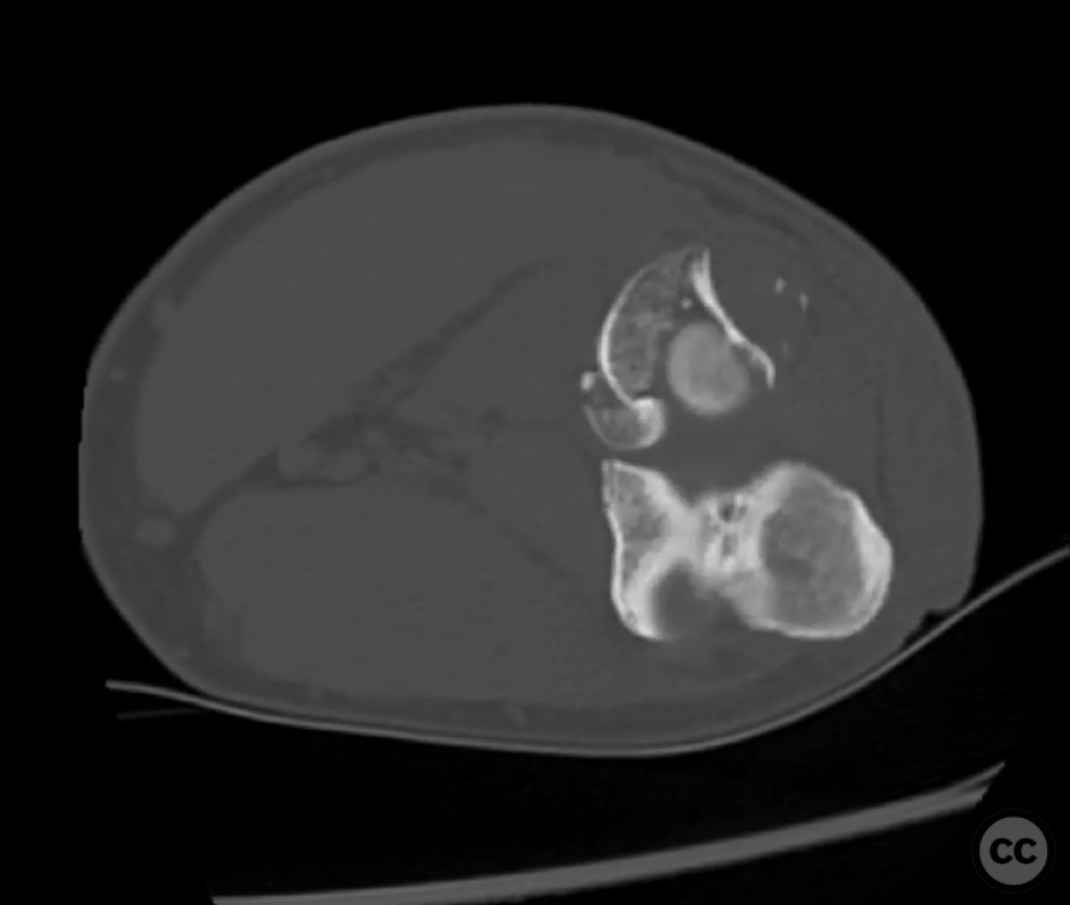
Clinical and radiological findings: A 54-year-old right hand dominant laborer sustained a fall from a height of 6 feet at work. The patient presented with an isolated, closed injury to the right upper extremity. There was no clear history of elbow dislocation requiring reduction, and the patient could not recall specific details of the injury mechanism. Initial clinical examination suggested a complex elbow injury pattern, raising suspicion for an Essex-Lopresti injury, characterized by potential interosseous membrane and distal radioulnar joint (DRUJ) disruption. Radiographic evaluation confirmed a comminuted four-part fracture of the radial head and neck. No coronoid process fracture was identified.
Preoperative Plan
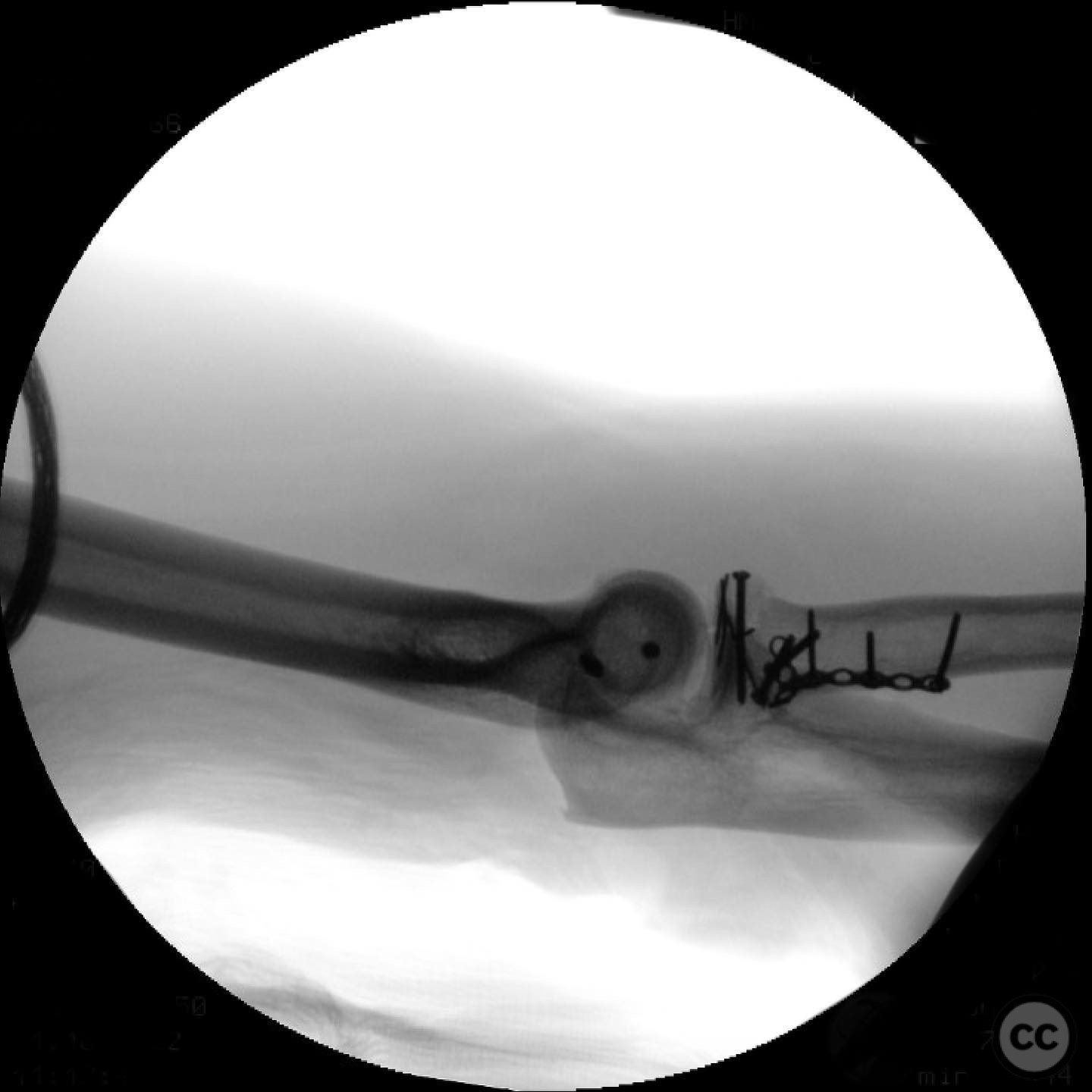
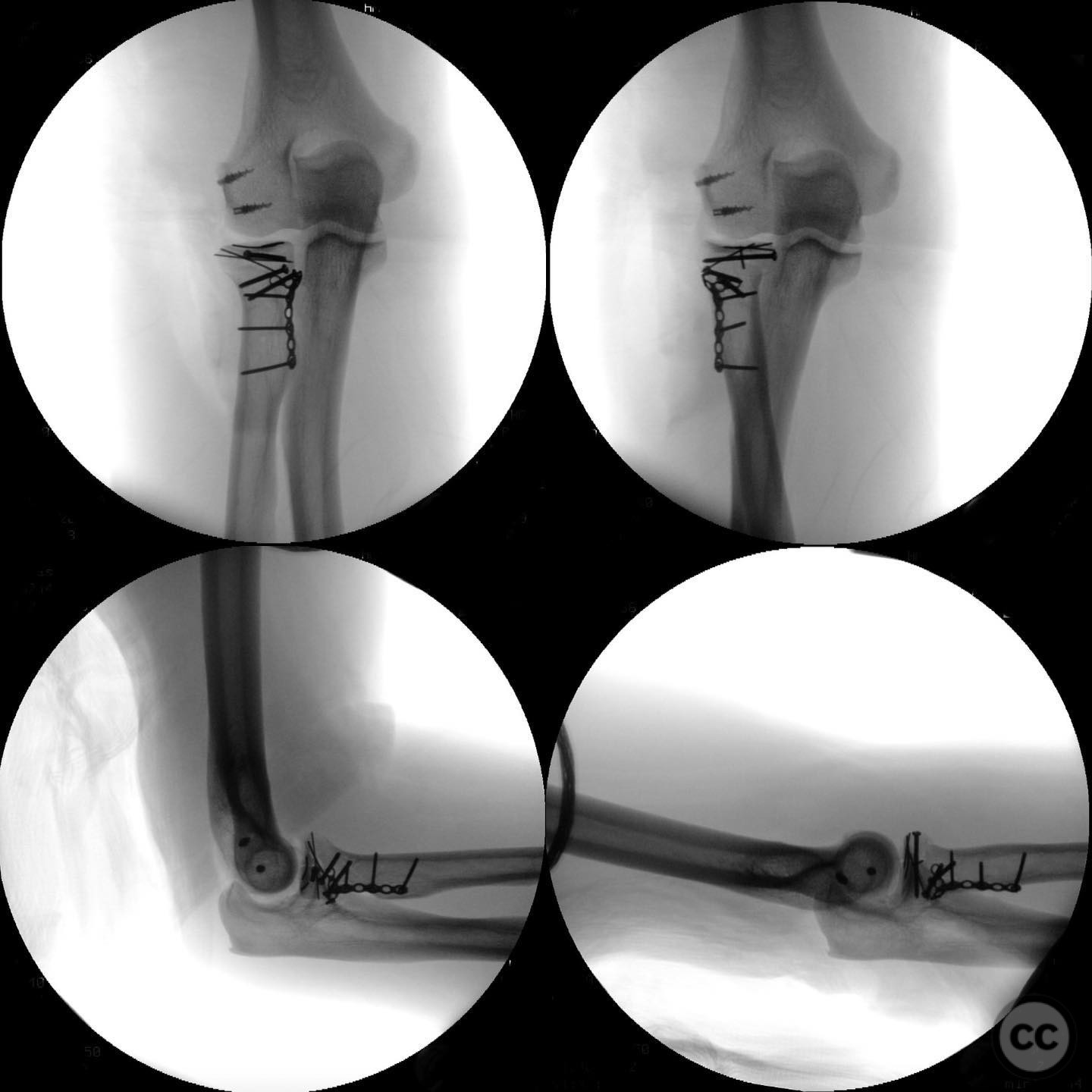
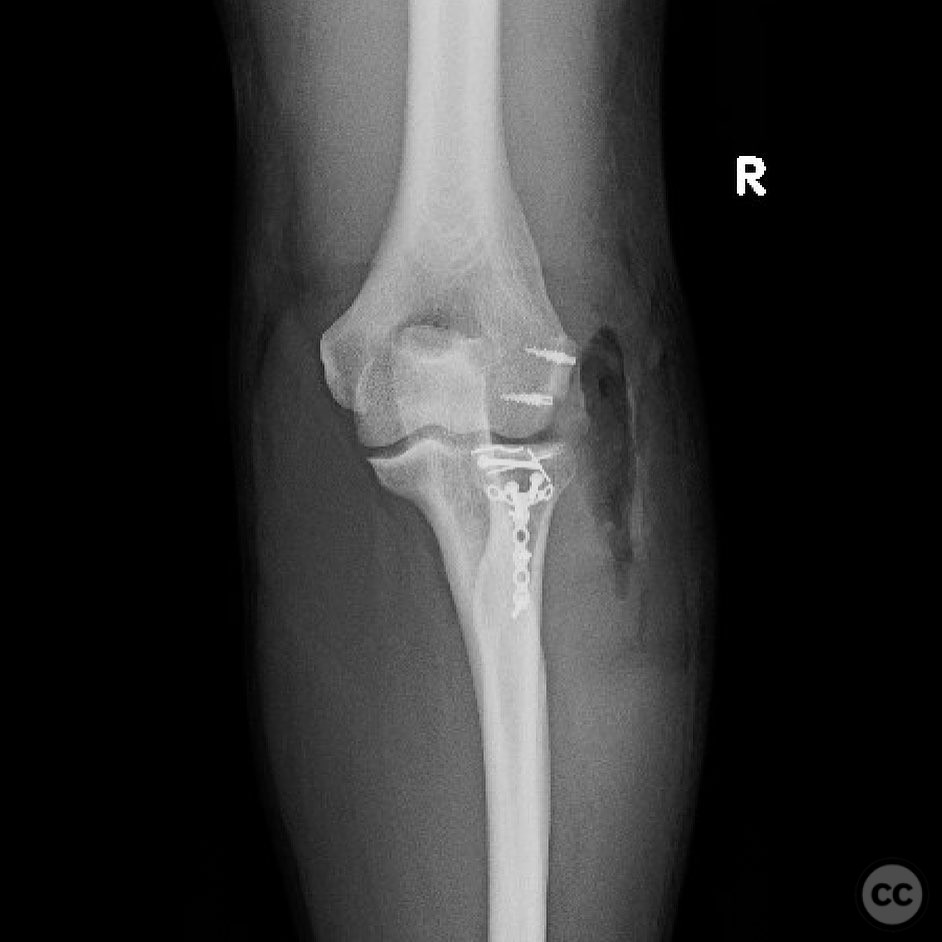
Planning remarks: The preoperative plan involved open reduction and internal fixation (ORIF) of the radial head and neck fracture using threaded K-wires, 1.5mm screws, 2.0mm screws, and a 1.5mm T-plate as a buttress on the neck. Additionally, repair of the lateral ulnar collateral ligament (LUCL) and common extensor origin was planned. Evaluation of the wrist for DRUJ stability was also considered.
Surgical Discussion
Patient positioning: The patient was positioned supine on the operating table with the affected arm placed on an arm board to allow for full access to the lateral aspect of the elbow.
Anatomical surgical approach: A lateral approach to the elbow was utilized, involving an incision over the lateral epicondyle. Dissection proceeded through the subcutaneous tissue to expose the extensor muscle origin, which was elevated to access the radial head and neck. The LUCL was identified and repaired following fixation of the radial head fracture.
Operative remarks:The surgeon noted that the radial head fracture required meticulous reconstruction due to its comminuted nature. Threaded K-wires were used for provisional fixation, followed by definitive fixation with 1.5mm and 2.0mm screws. A 1.5mm T-plate was applied to the radial neck as a buttress to enhance stability. The LUCL and common extensor origin were repaired using non-absorbable sutures. Intraoperative assessment of DRUJ stability was performed, and no immediate intervention was required for the wrist.
Postoperative protocol: Postoperatively, a specific motion protocol was initiated at one week, continuing through week six. An orthoplast splint was applied when not performing exercises to protect the repair while allowing controlled motion.
Follow up: Not specified.
Orthopaedic implants used: Threaded K-wires, 1.5mm screws, 2.0mm screws, 1.5mm T-plate.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 323 times
12 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Complex Essex-Lopresti Variant: Comminuted Radial Head Fracture Managed with ORIF and LUCL Reconstruction. Journal of Orthopaedic Surgery and Traumatology. Case Report 17185640 Published Online Jul 12 2025.