 and tachycardic in the ED_ no head_ chest or belly inju(.jpg)
 and tachycardic in the ED_ no head_ chest or belly inj_1.jpg)
 and tachycardic in the ED_ no head_ chest or belly inj_2.jpg)
 and tachycardic in the ED_ no head_ chest or belly inj_3.jpg)
 and tachycardic in the ED_ no head_ chest or belly inj_4.jpg)
 and tachycardic in the ED_ no head_ chest or belly inj_5.jpg)
 and tachycardic in the ED_ no head_ chest or belly inj_6.jpg)
 and tachycardic in the ED_ no head_ chest or belly inj_7.jpg)








Polytrauma Management with Femur, Pilon, Olecranon, and Fibula Fractures
Score and Comment on this Case
Clinical Details
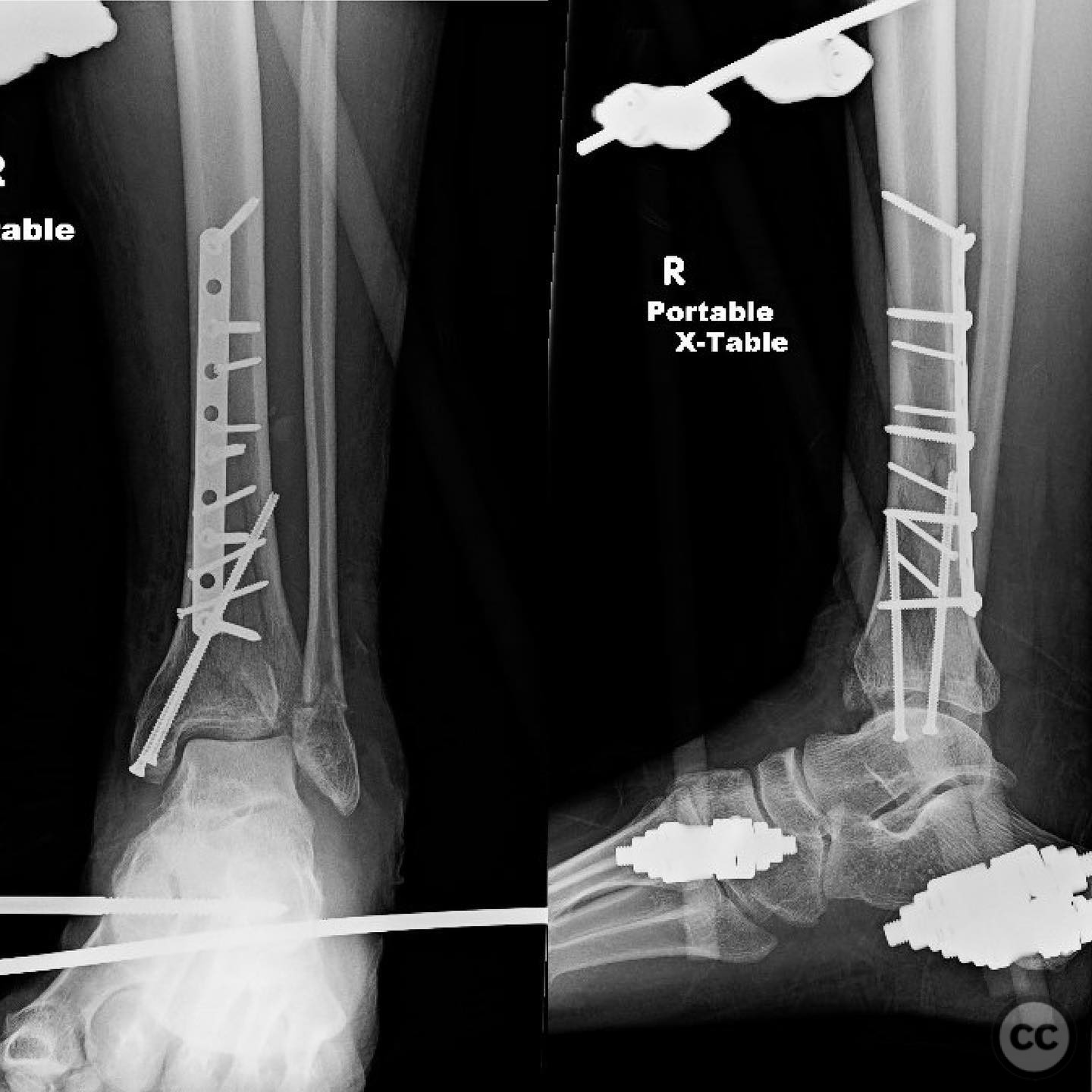
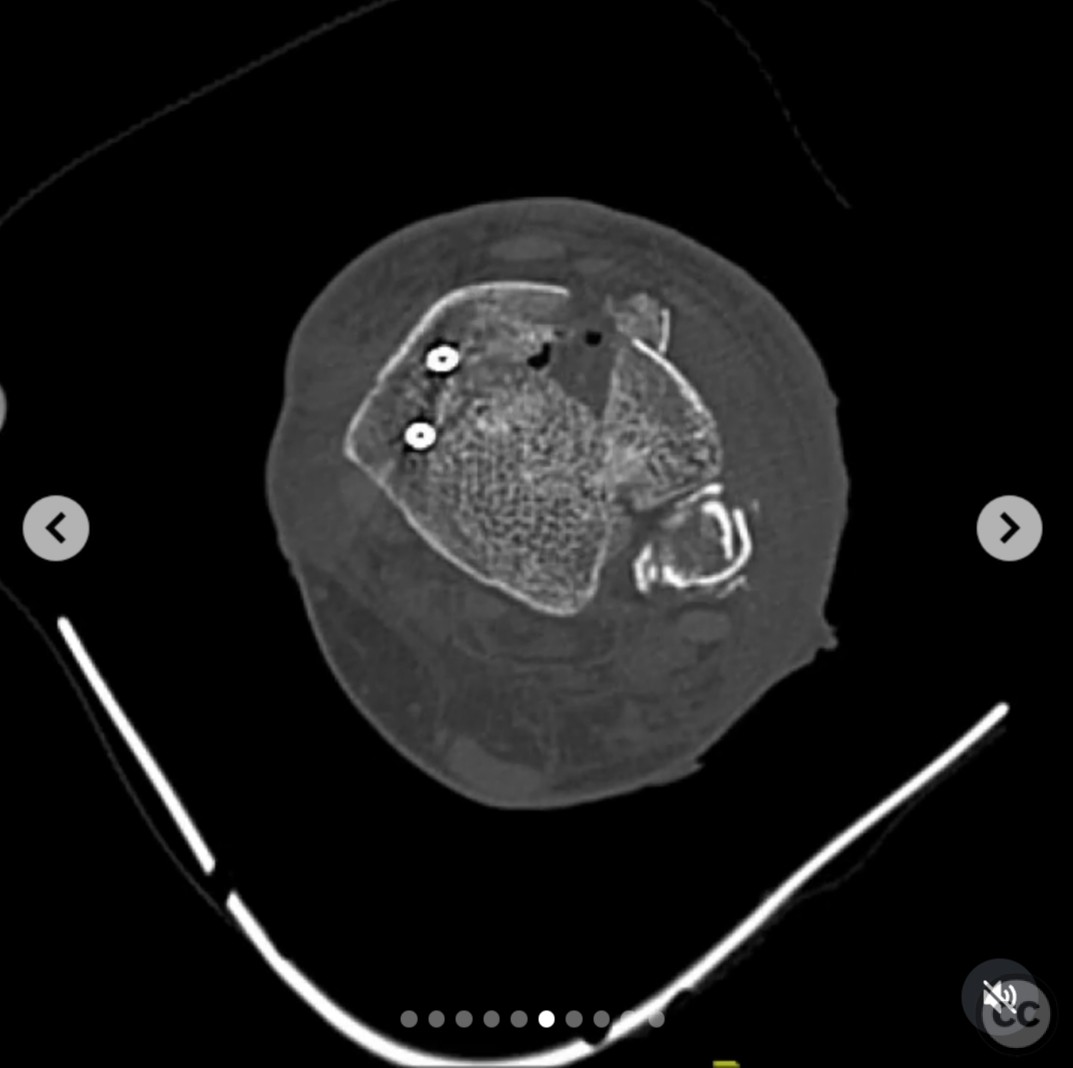
Clinical and radiological findings: A 33-year-old male sustained multiple skeletal injuries after a 30-foot fall at a party. Initial presentation in the emergency department revealed hypoxia (SaO2 83% on room air, 91% on 6L oxygen) and tachycardia, with stable blood pressure. Laboratory findings included lactate of 2.0 mmol/L, hematocrit of 33%, and platelet count of 245 x 10^9/L. The patient tested positive for methamphetamine, heroin, and benzodiazepines. No head, chest, or abdominal injuries were identified. All skeletal injuries were closed fractures. The patient had a femoral shaft fracture, a pilon fracture, an olecranon fracture, and a fibular fracture.
Preoperative Plan
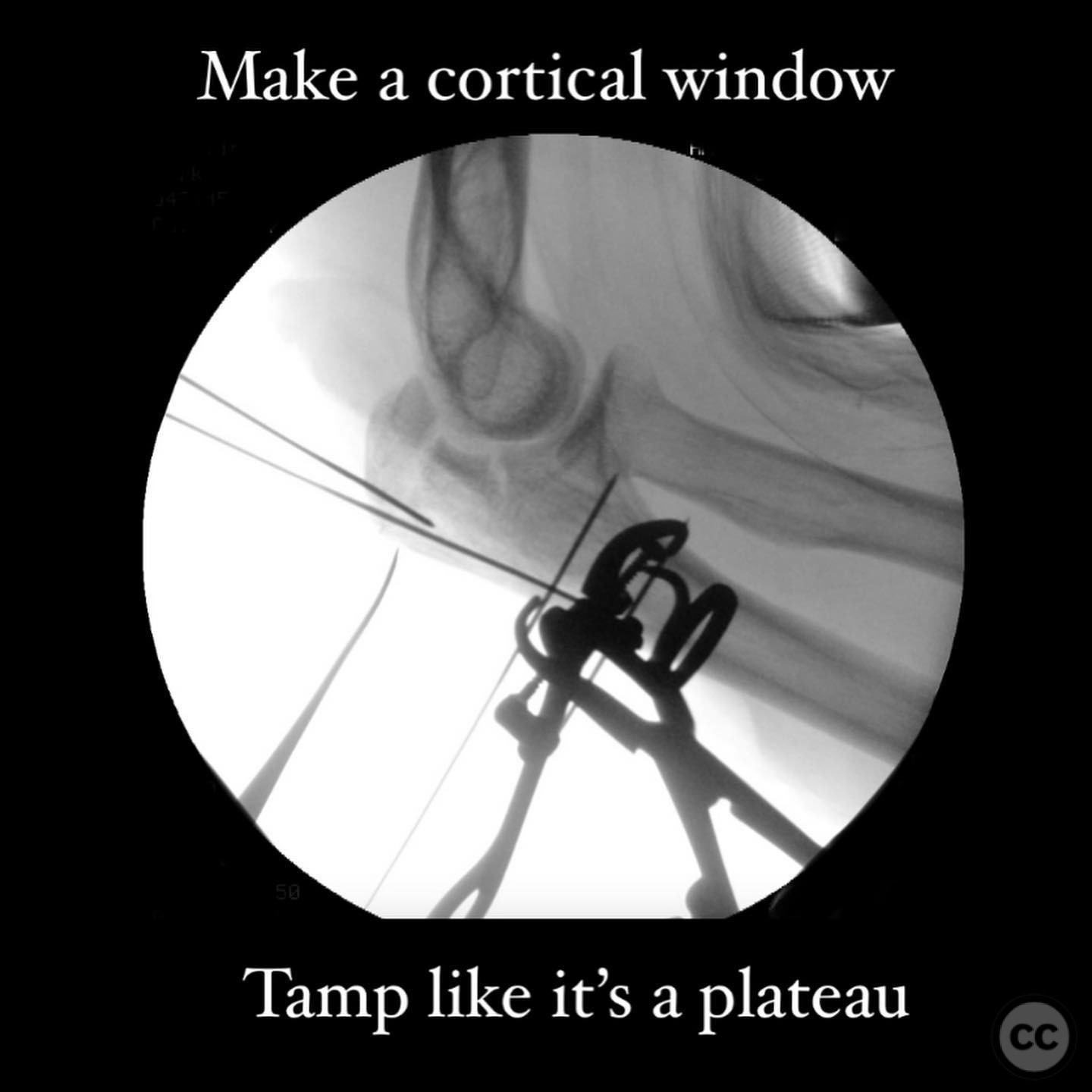
Planning remarks: The preoperative plan involved addressing the femoral shaft fracture first with an open reduction and internal fixation using biologically friendly cerclage and trochanteric entry reamed antegrade recon nailing. The pilon fracture was approached in two stages: initially via a posteromedial approach for early stabilization and later definitive fixation. The olecranon fracture required a cortical window osteotomy for fragment elevation and bone grafting before standard fixation. The fibula was planned for length restoration and alignment correction with a bridge plate.
Surgical Discussion
Patient positioning: For the femoral fracture, the patient was positioned laterally to facilitate the open reduction and nailing procedure.
Anatomical surgical approach: The femoral fracture was approached via a lateral incision with trochanteric entry for antegrade nailing. The pilon fracture was initially spanned and scanned, followed by a posteromedial approach for early stabilization. Definitive fixation of the pilon was performed through an anteromedial approach with careful disimpaction and bone grafting. The olecranon was accessed through a posterior approach with a cortical window osteotomy to elevate the impacted fragment.
Operative remarks:The surgeon noted the importance of addressing the patient's respiratory status due to hypoxia and potential benzodiazepine withdrawal, necessitating intubation and systemic management. The femoral fracture was stabilized first to address the major long bone injury. The pilon fracture was managed using an early C to B strategy, allowing for straightforward definitive fixation after soft tissue defervescence. The olecranon required innovative access through a cortical window due to lack of typical coronal plane split. The fibula was shortened by the time of definitive treatment, necessitating length restoration with a bridge plate.
Postoperative protocol: Postoperative rehabilitation included maintaining non-weight bearing status initially, progressing to partial weight bearing as tolerated based on individual fracture healing and soft tissue recovery.
Follow up: Not specified.
Orthopaedic implants used: Trochanteric entry reamed antegrade recon nail, biologically friendly cerclage wire, provisional wires, 2.0 rim plate, 3.5 anterolateral plate, bridge plate for fibula.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 261 times
12 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Polytrauma Management with Femur, Pilon, Olecranon, and Fibula Fractures. Journal of Orthopaedic Surgery and Traumatology. Case Report 1638733 Published Online Jul 12 2025.