






Scapular Body and Glenoid Neck Fracture with Significant Lateralization.
Score and Comment on this Case
Clinical Details
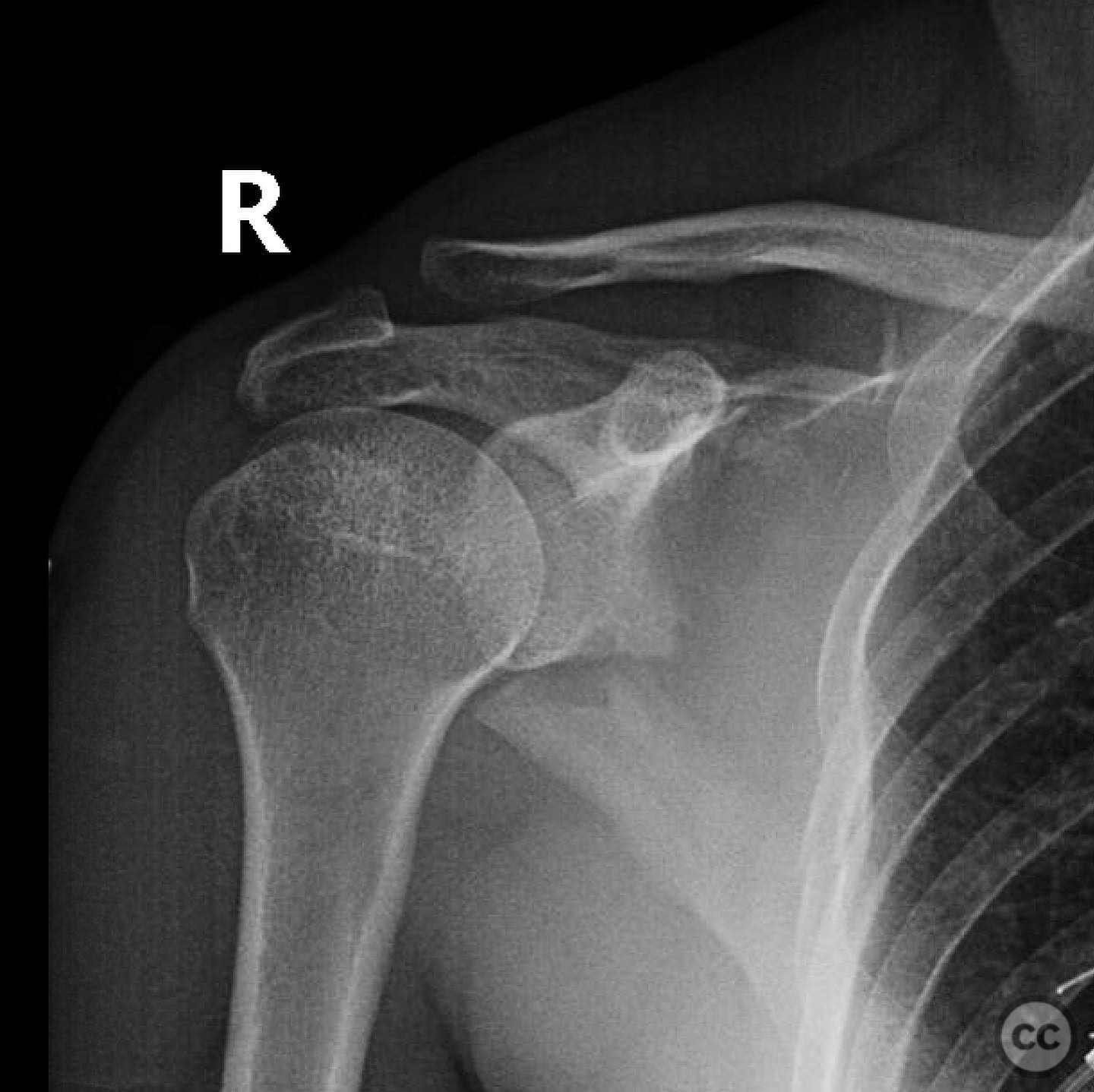
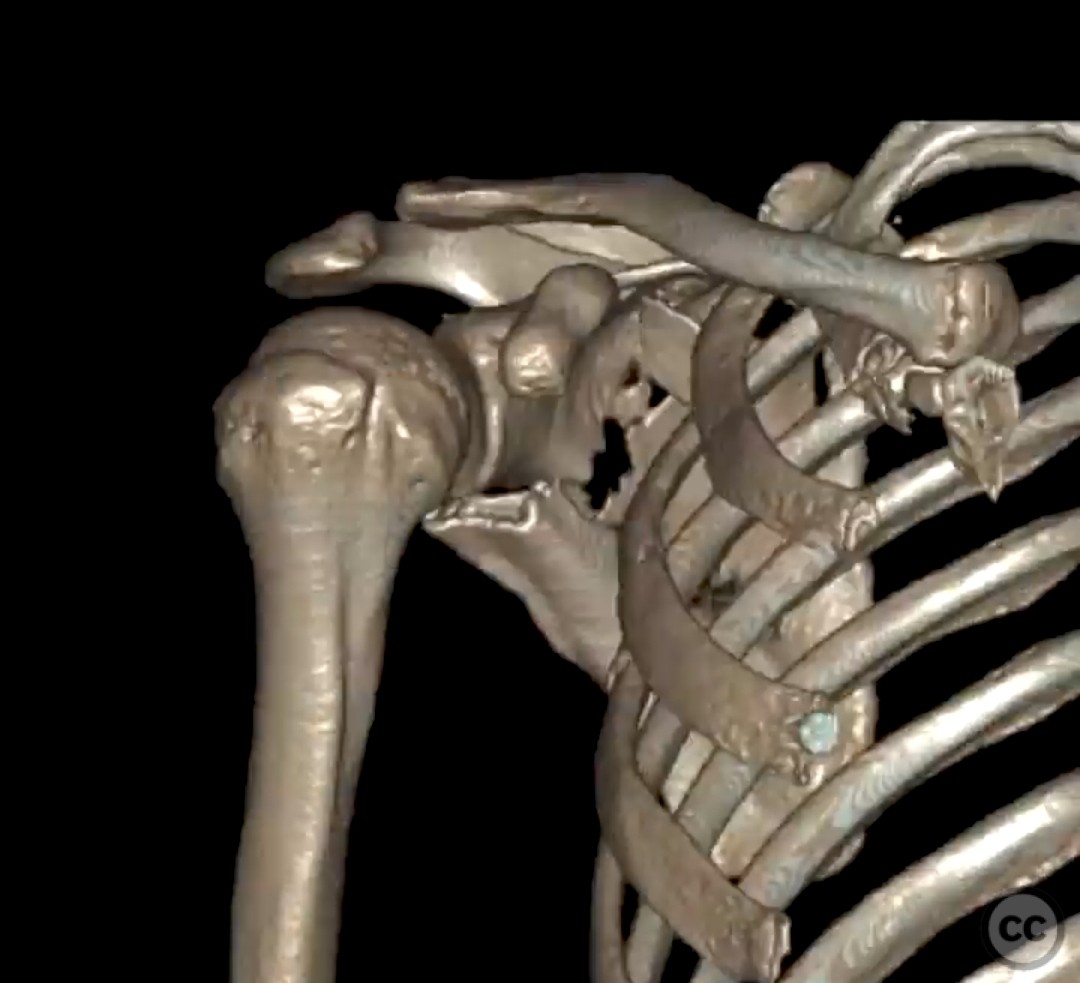
Clinical and radiological findings: A 32-year-old male, active and healthy, sustained a fracture of the glenoid neck and scapular body following a mountain biking accident. The patient also presented with associated rib fractures. Radiological assessment, including 3D reconstruction, revealed lateralization of the scapular body between 3 and 4 cm. The glenopolar angle was normal, and there was no significant angulation of the scapular body or articular incongruity of the glenoid.
Preoperative Plan
Planning remarks: The preoperative plan involved a posterior approach to the scapula to address the significant lateralization of the scapular body. The surgical objective was to restore anatomical alignment and prevent potential rotator cuff dysfunction.
Surgical Discussion
Patient positioning: The patient was positioned in a lateral decubitus position with the affected side up, allowing optimal access to the posterior aspect of the scapula.
Anatomical surgical approach: A posterior approach was utilized, involving a longitudinal incision along the medial border of the scapula. Subperiosteal dissection was performed to expose the scapular body and glenoid neck. Care was taken to protect the suprascapular nerve during exposure.
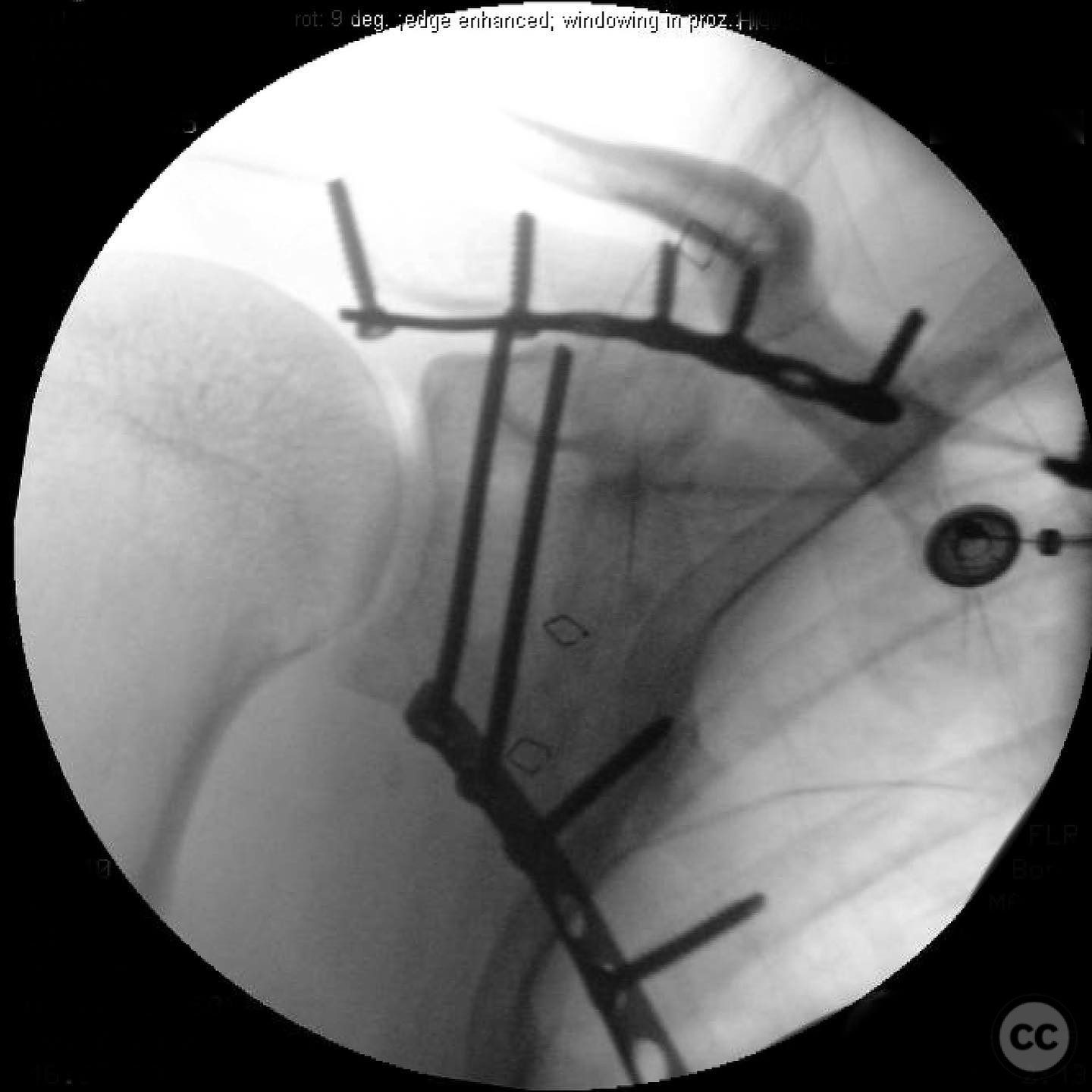
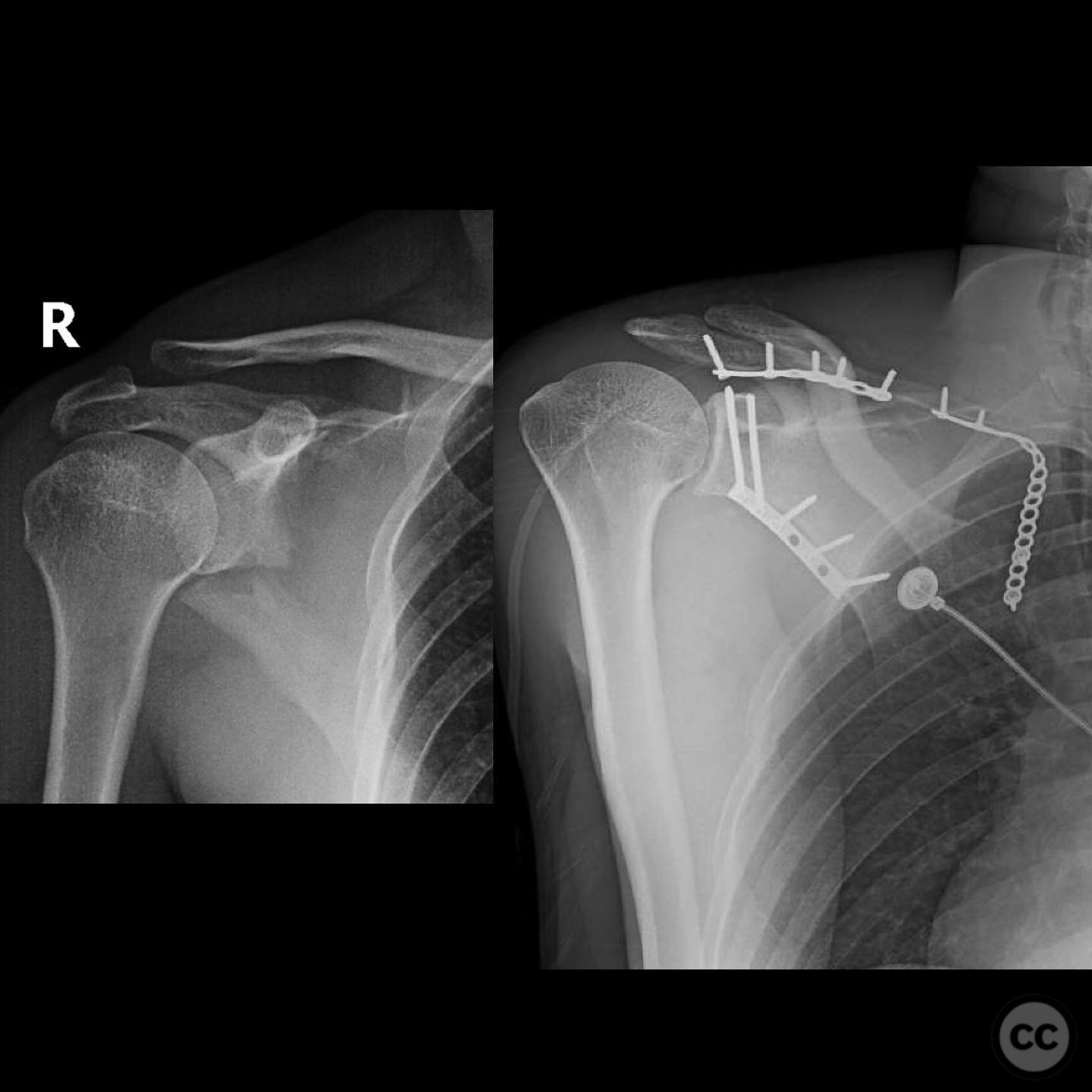
Operative remarks:The surgeon noted that the degree of lateralization was significant, necessitating careful reduction and fixation to restore proper scapular alignment. Intraoperative fluoroscopy was used to confirm reduction. The fixation was achieved using plate and screw constructs to stabilize the fracture fragments.
Postoperative protocol: Postoperatively, the patient was placed in a shoulder immobilizer for 4 weeks. Passive range of motion exercises were initiated at 2 weeks post-surgery, progressing to active-assisted exercises by 6 weeks. Strengthening exercises were introduced at 8 weeks, with a focus on restoring full shoulder function.
Follow up: Not specified.
Orthopaedic implants used: Plate and screw constructs for scapular fixation.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 341 times
14 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Scapular Body and Glenoid Neck Fracture with Significant Lateralization.. Journal of Orthopaedic Surgery and Traumatology. Case Report 16015563 Published Online Jul 14 2025.