

.jpg)
.jpg)
Complex Unilateral Iliac Fracture with Contralateral Sacral and Parasymphyseal Ramus Fractures: ORIF and Percutaneous Fixation
Score and Comment on this Case
Clinical Details
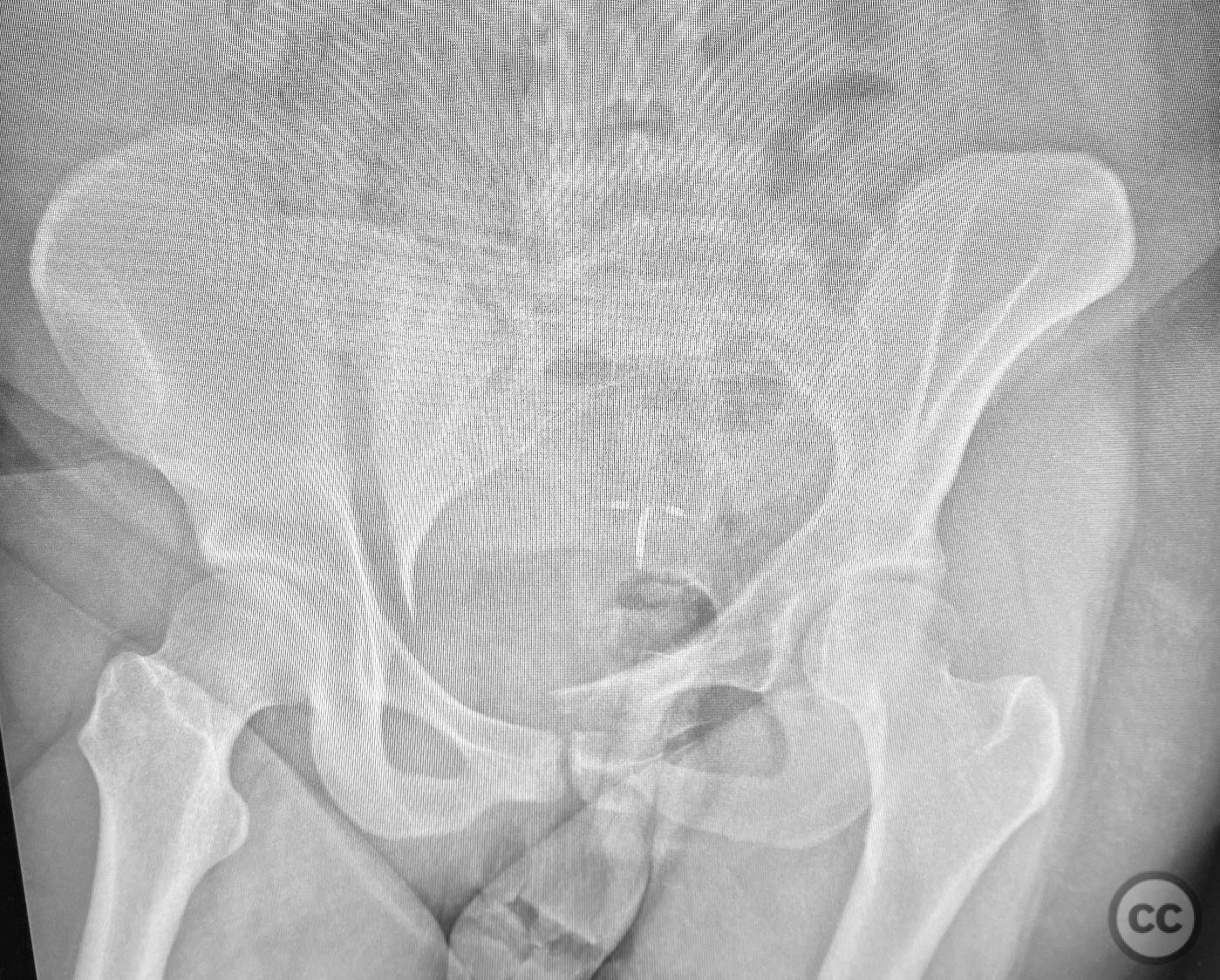
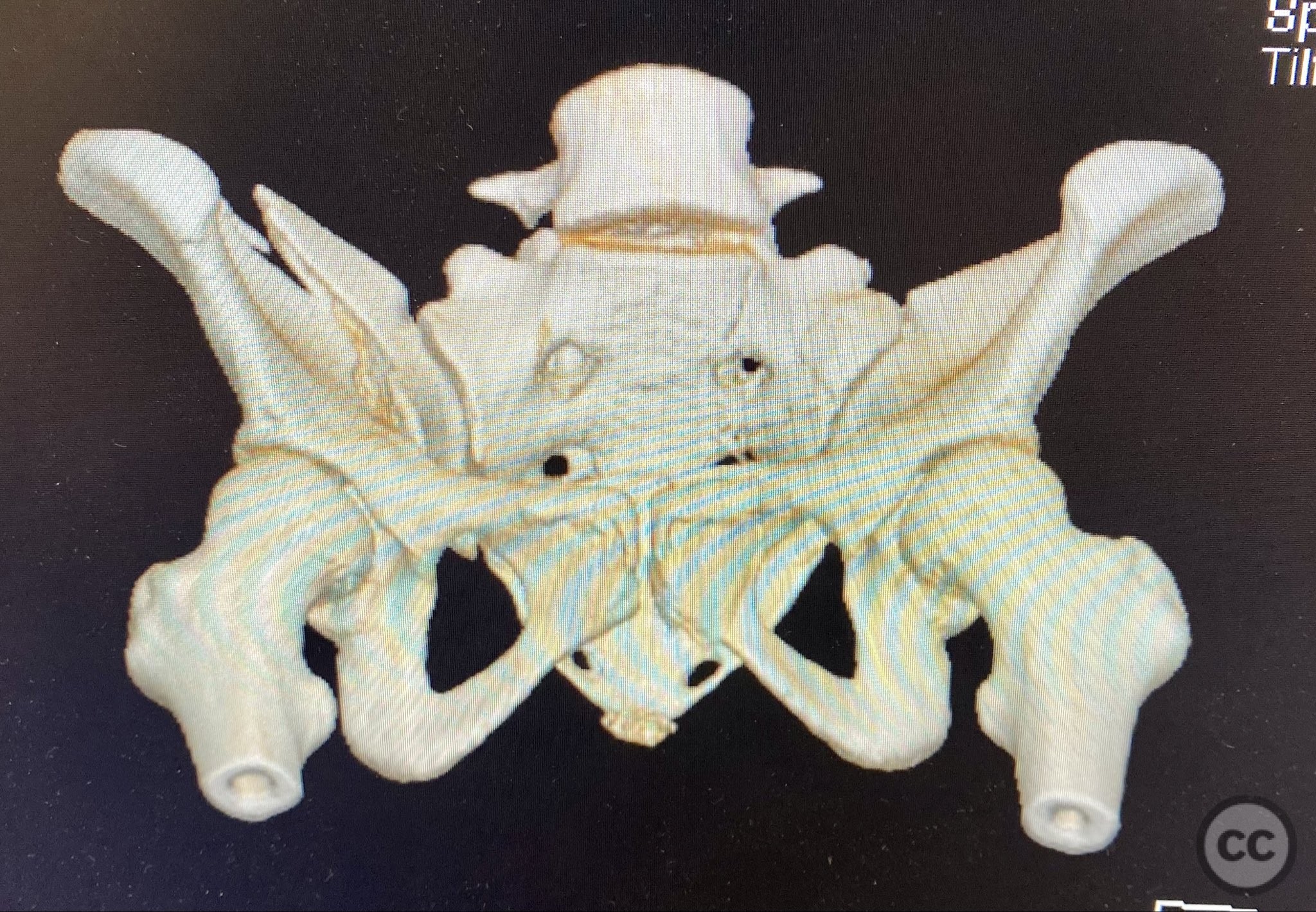
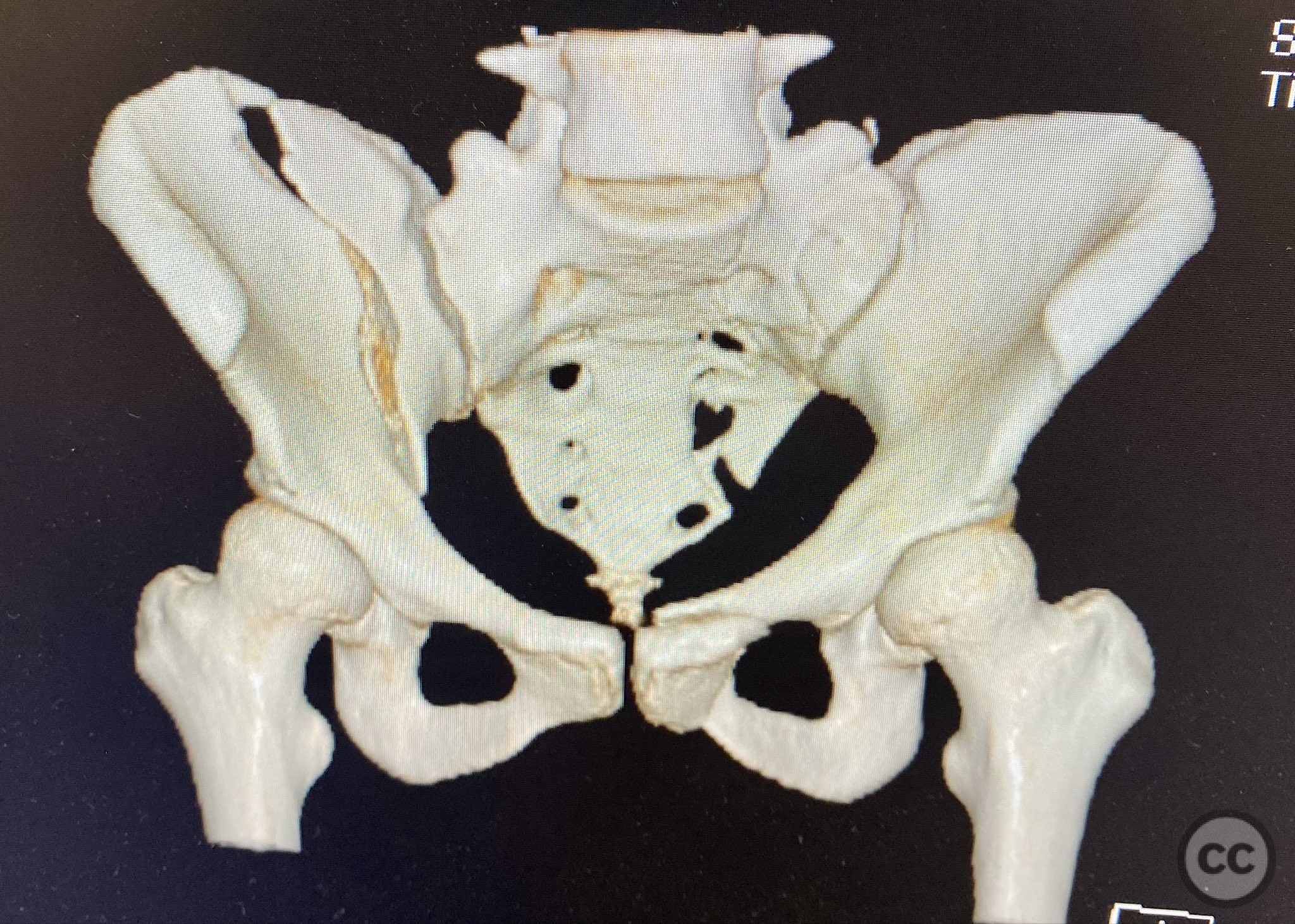
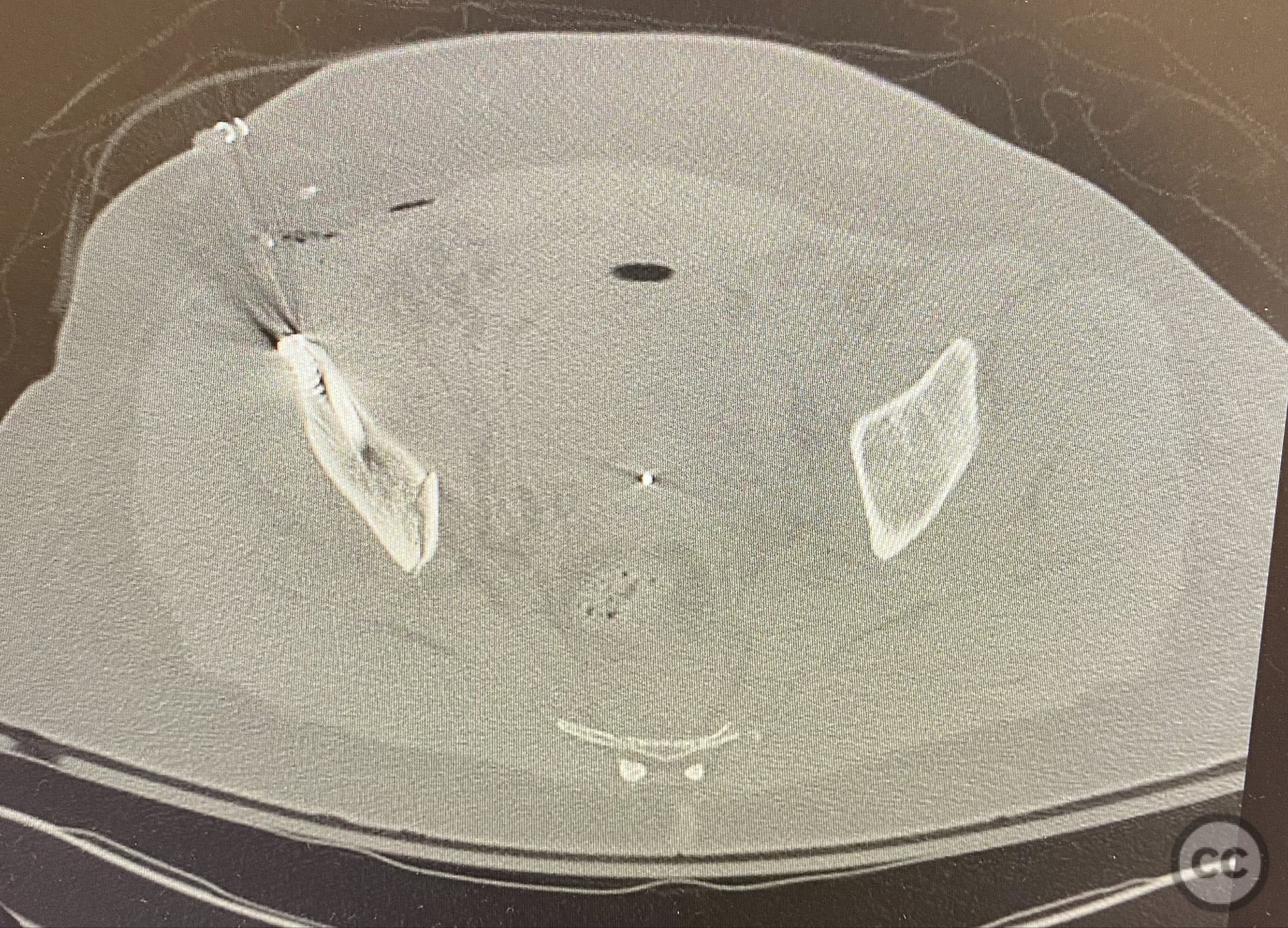
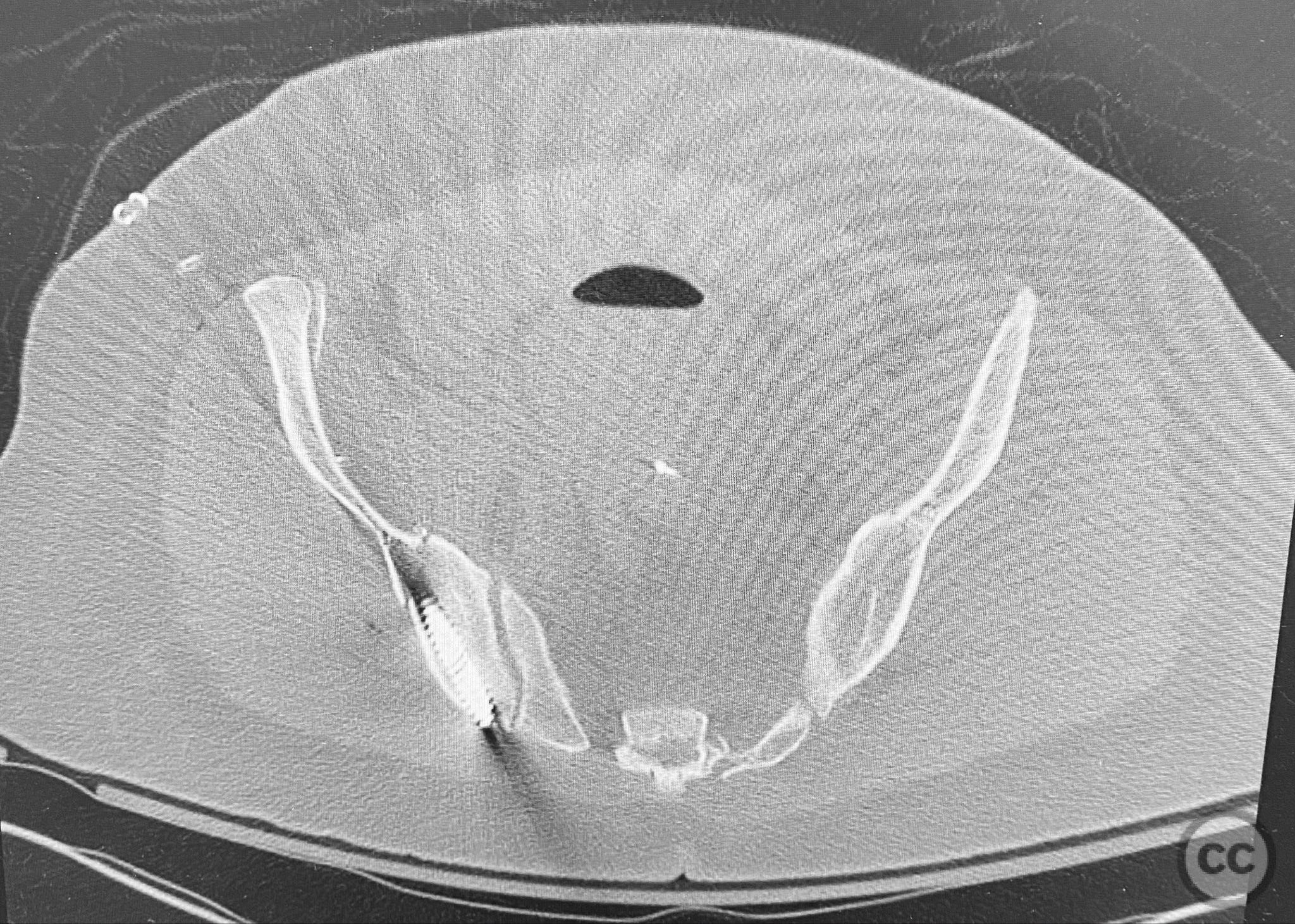
Clinical and radiological findings: The patient presented following trauma with an unusual, significantly displaced right iliac fracture, accompanied by left-sided sacral and parasymphyseal ramus fractures. Initial AP pelvic radiography demonstrated the complex injury pattern. CT imaging provided detailed characterization of the iliac and sacral fractures, including assessment of displacement, bone quality, soft tissue status, and overall body habitus. No neurovascular compromise was reported. AO/OTA classification: Right iliac fracture 61B2.3 (partial unstable, lateral compression injury), left sacral fracture Denis zone I, left parasymphyseal ramus fracture.
Preoperative Plan
Planning remarks: The preoperative plan included initial application of bilateral distal femoral traction to achieve provisional reduction, particularly targeting the sacral displacement. Definitive surgical management consisted of percutaneous stabilization of the left sacral fracture and open reduction with internal fixation (ORIF) of the right iliac fracture via an anterior approach, with planned placement of pelvic brim cancellous screws.
Surgical Discussion
Patient positioning: The patient was positioned supine on a radiolucent table to facilitate fluoroscopic imaging and allow access for both percutaneous and open approaches to the pelvis.
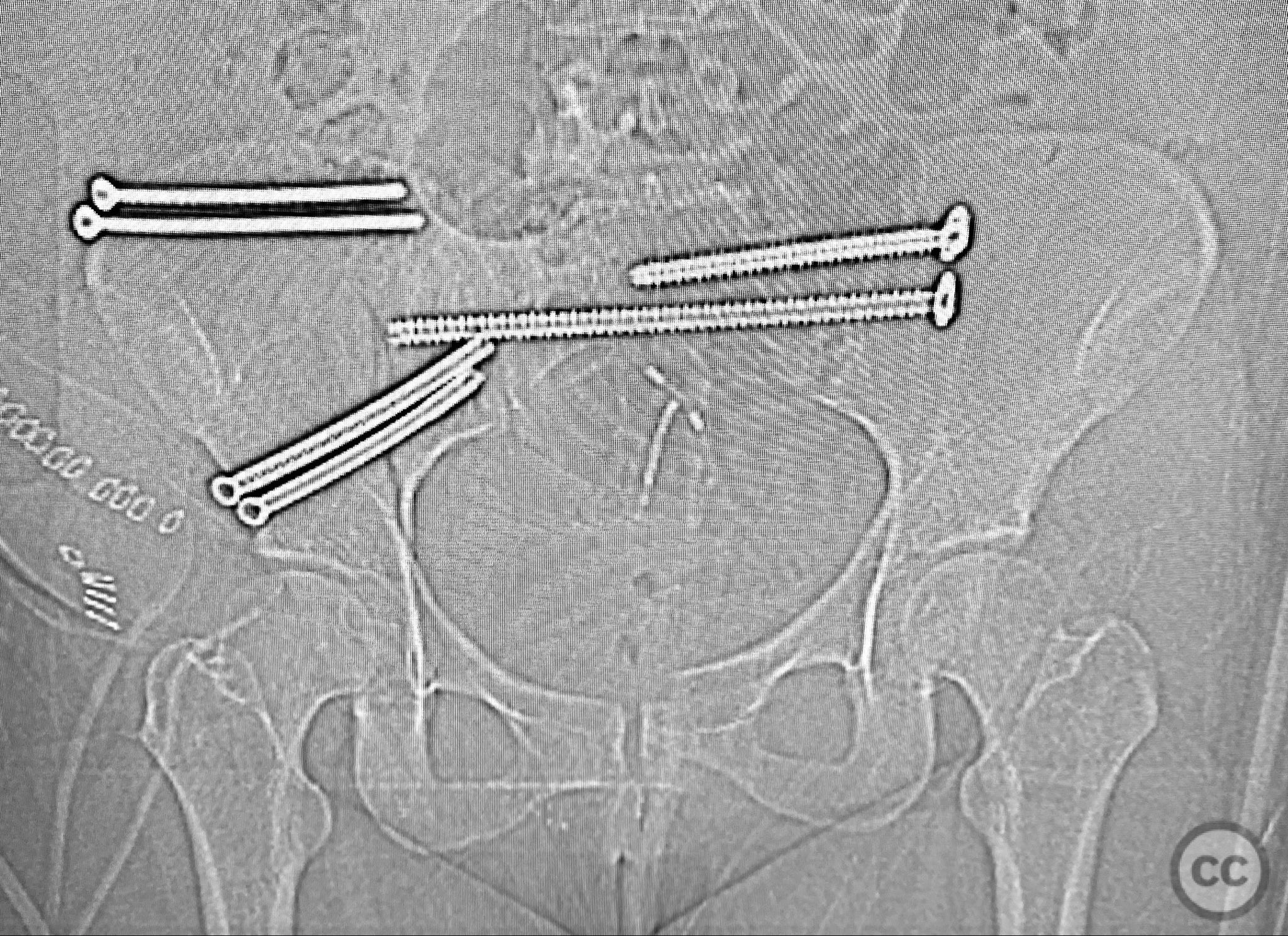
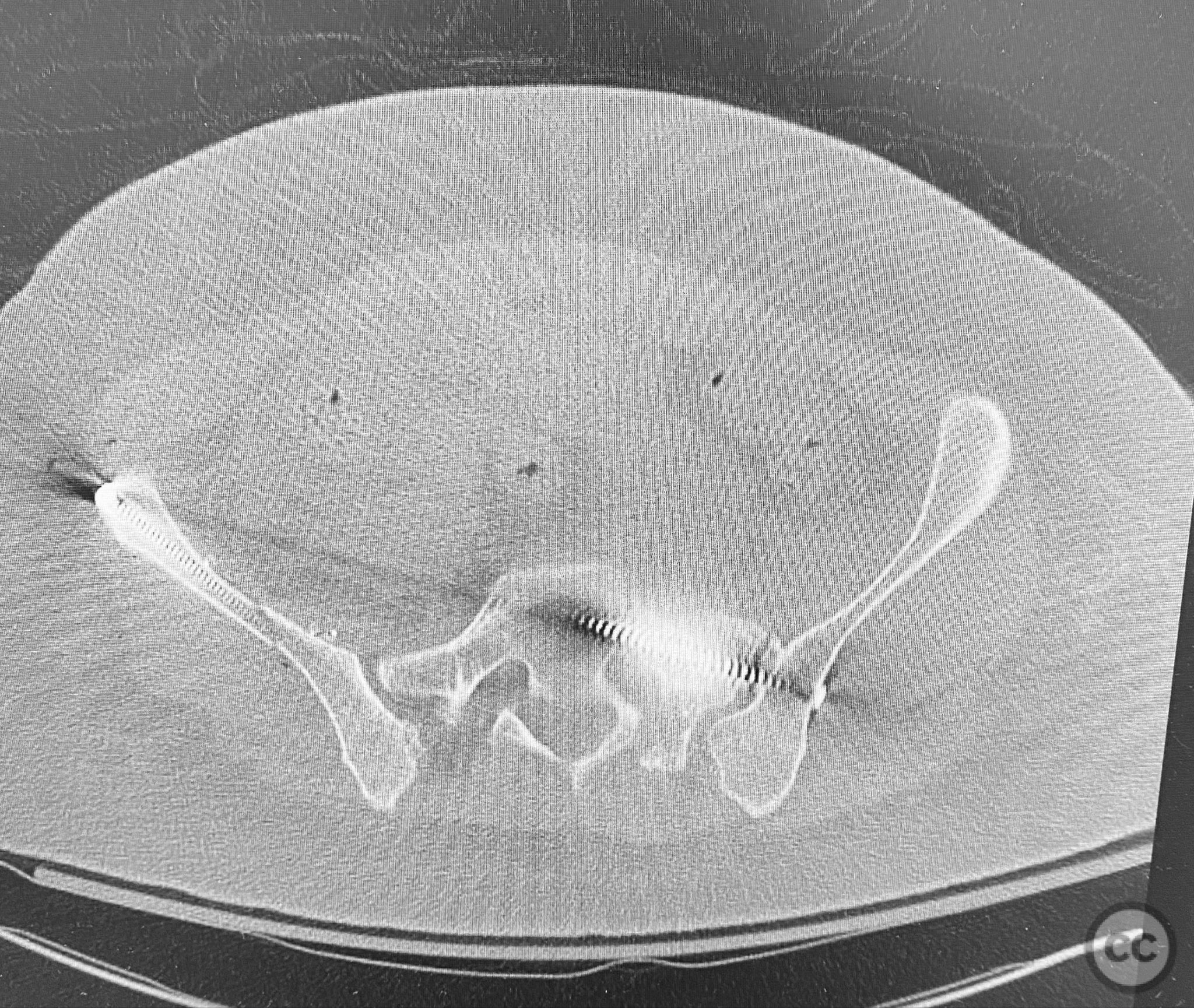
Anatomical surgical approach: A standard anterior ilioinguinal approach was utilized for the right iliac fracture. Dissection proceeded through the skin and subcutis, with identification and protection of the lateral femoral cutaneous nerve. The external oblique aponeurosis was incised, and the iliacus muscle was elevated subperiosteally from the internal iliac fossa to expose the fracture site. Reduction was achieved under direct visualization, followed by internal fixation with a contoured plate and pelvic brim cancellous screws, ensuring all implants were contained within the osseous fixation pathway. The left sacral fracture was stabilized percutaneously under fluoroscopic guidance.
Operative remarks:Bilateral distal femoral traction resulted in excellent reduction of the sacral fracture but did not adequately reduce the iliac displacement. Percutaneous fixation of the sacrum was performed first, followed by open reduction of the iliac fracture. Intraoperative imaging confirmed that all implants were fully contained within the available osseous corridors, avoiding extraosseous penetration. The complexity of the iliac fracture required careful anatomical reduction and implant placement along the pelvic brim.
Postoperative protocol: Postoperatively, the patient was maintained non-weight bearing on the affected side for six weeks, with progressive mobilization as tolerated. Early passive and active-assisted range of motion exercises for the hip and knee were initiated immediately postoperatively.
Follow up: Not specified
Orthopaedic implants used: Pelvic brim contoured plate, cancellous screws, percutaneous sacral screw(s)
Search for Related Literature


Industry Sponsership
contact us for advertising opportunities
Article viewed 286 times
12 Sep 2025
Add to Bookmarks
Full Citation
Cite this article:
Routt, ML. (2025). Complex Unilateral Iliac Fracture with Contralateral Sacral and Parasymphyseal Ramus Fractures: ORIF and Percutaneous Fixation. Journal of Orthopaedic Surgery and Traumatology. Case Report 1436993 Published Online Sep 12 2025.