















When the Talus Won’t Budge: A Battle Against a Locked Subtalar Dislocation"
Score and Comment on this Case
Clinical Details
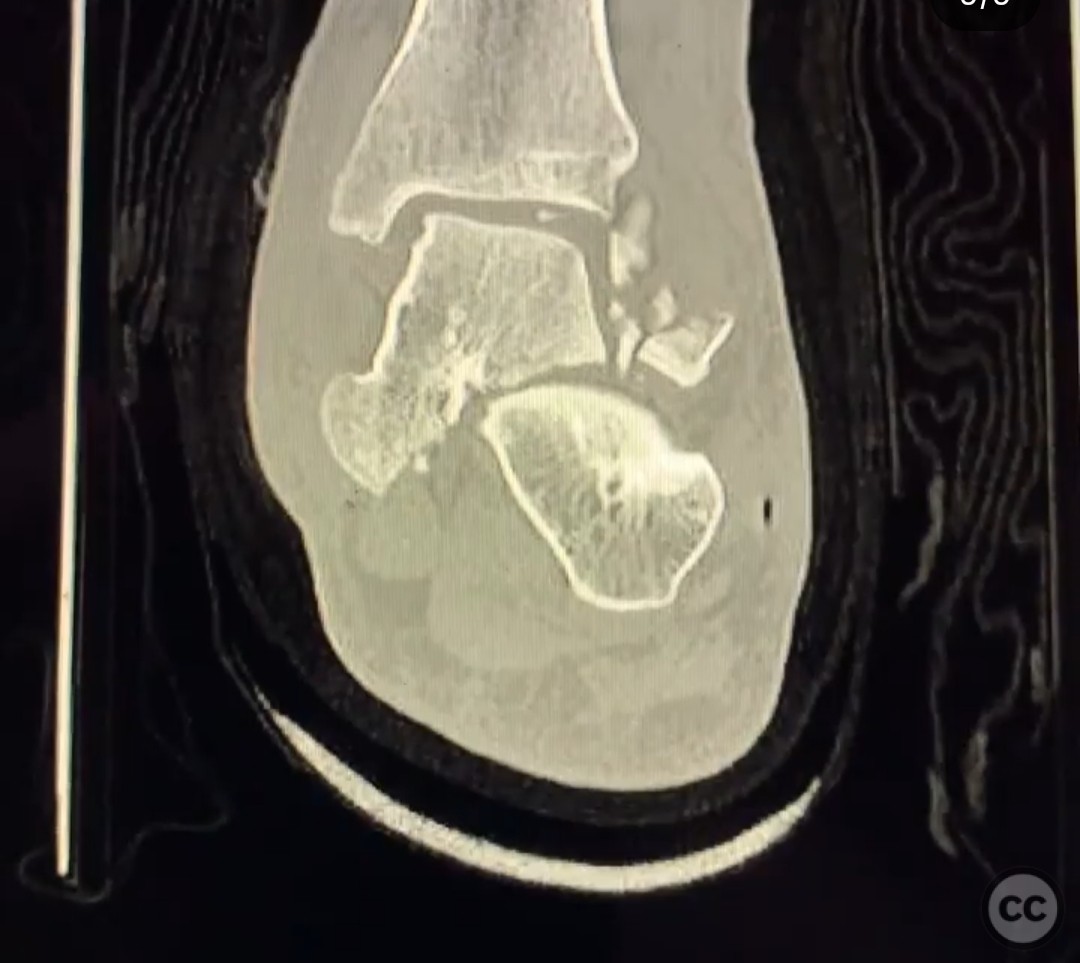
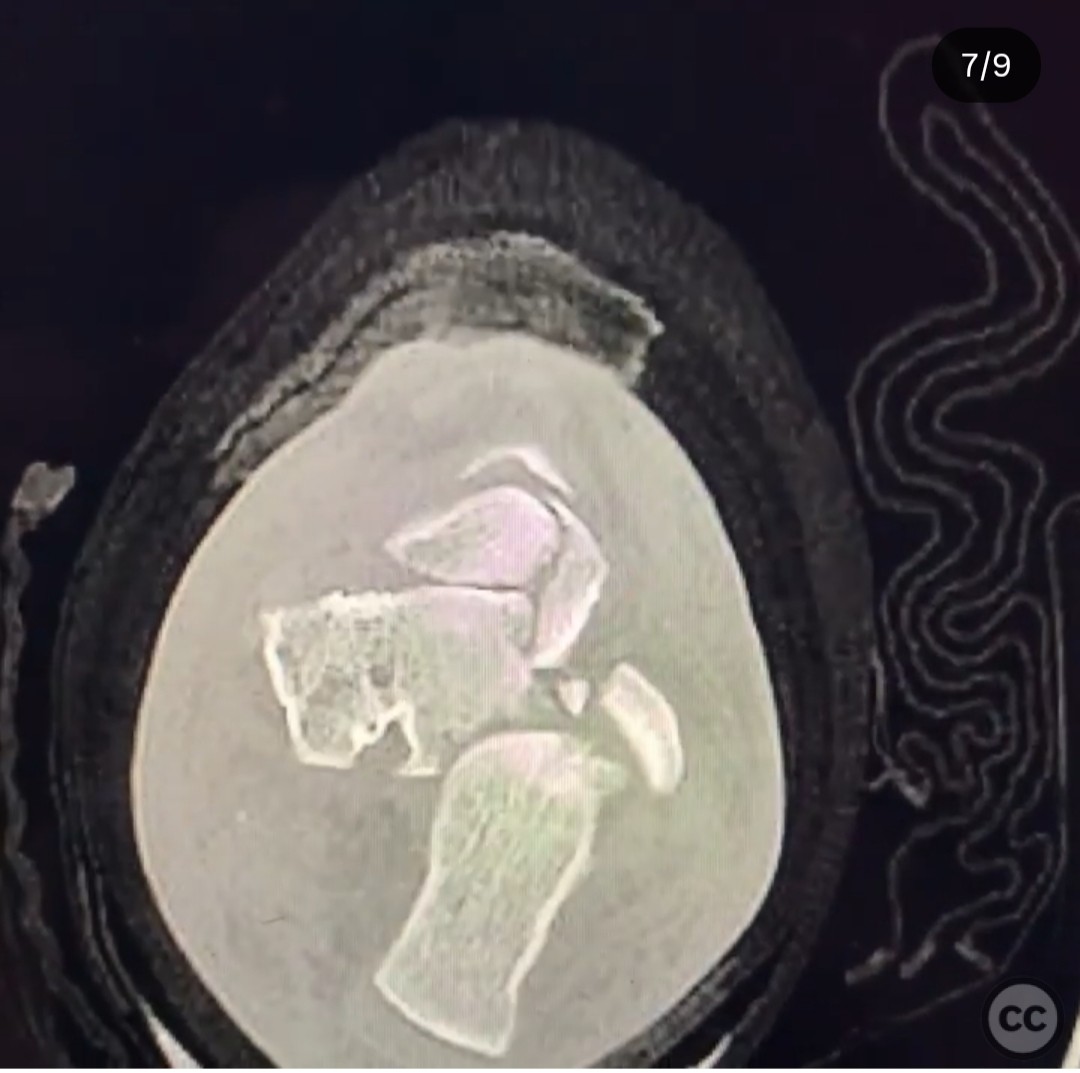
Clinical and radiological findings: A 28-year-old male sustained a complex lateral subtalar dislocation following a motorcycle crash. Initial management at a level 3 trauma center involved failed closed and open reduction attempts through a dorsal incision. The patient was transferred to our trauma center after 2 days with the talus still dislocated. Radiographic evaluation confirmed the dislocation with obstruction by the flexor hallucis longus, tibial nerve and artery, flexor digitorum longus, and posterior tibial tendon. The talar head was buttonholed through the plantar talonavicular capsule.
Preoperative Plan
Planning remarks: The preoperative plan involved a posteromedial approach to address the obstructing tendons and reduce the talar head from its buttonhole position through the plantar talonavicular capsule.
Surgical Discussion
Patient positioning: The patient was positioned supine with the affected limb externally rotated to facilitate access to the posteromedial aspect of the ankle.
Anatomical surgical approach: A posteromedial approach was utilized, involving an incision along the posterior border of the medial malleolus. Careful dissection was performed to retract the flexor retinaculum and expose the obstructing tendons, allowing for reduction of the talar head through the buttonhole in the plantar talonavicular capsule.
Operative remarks:The reduction was challenging due to the buttonhole entrapment of the talar head. Initial attempts with external fixation and various instruments were unsuccessful. Successful reduction was achieved by addressing the buttonhole entrapment directly through the posteromedial approach. The subtalar joint was noted to be in good condition post-reduction, although the risk of avascular necrosis remains high.
Postoperative protocol: Postoperative rehabilitation included non-weight bearing with immobilization in a splint for 6 weeks, followed by gradual weight-bearing as tolerated with physical therapy focusing on range of motion and strengthening exercises.
Follow up: Not specified
Orthopaedic implants used: External fixator, 2.5mm Schanz pins
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 281 times
20 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). When the Talus Won’t Budge: A Battle Against a Locked Subtalar Dislocation". Journal of Orthopaedic Surgery and Traumatology. Case Report 14085824 Published Online Jul 20 2025.