

.jpg)




Combined Symphysis Pubis Disruption and Incomplete Left Sacroiliac Joint Injury in an Adult
Score and Comment on this Case
Clinical Details
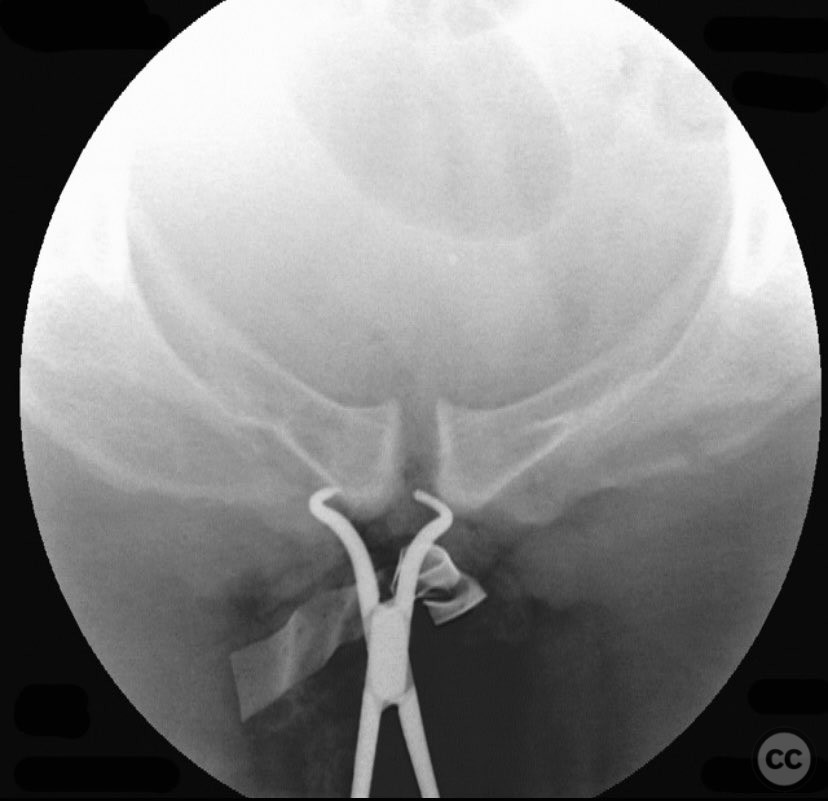
Clinical and radiological findings: An adult patient sustained traumatic disruption of the symphysis pubis and an incomplete left sacroiliac (SI) joint injury. Initial radiographs and pelvic CT scan (performed without circumferential pelvic wrapping) demonstrated a widened symphysis pubis and an incomplete disruption of the left SI joint. The CT scan further provided information regarding bone quality, upper sacral morphology, patient body habitus, and vascular anatomy. No additional pelvic ring injuries were identified. AO/OTA classification: 61-B2.1 (lateral compression injury with incomplete posterior disruption).
Preoperative Plan
Planning remarks: The preoperative plan included open reduction and internal fixation of the symphysis pubis via an anterior approach, with provisional reduction using a pelvic reduction clamp. Indirect reduction of the SI joint was anticipated via anterior stabilization; however, preparation for percutaneous iliosacral screw fixation was considered should indirect reduction prove inadequate.
Surgical Discussion
Patient positioning: The patient was positioned supine on a radiolucent operating table to facilitate both anterior open exposure and fluoroscopic access for percutaneous posterior fixation.
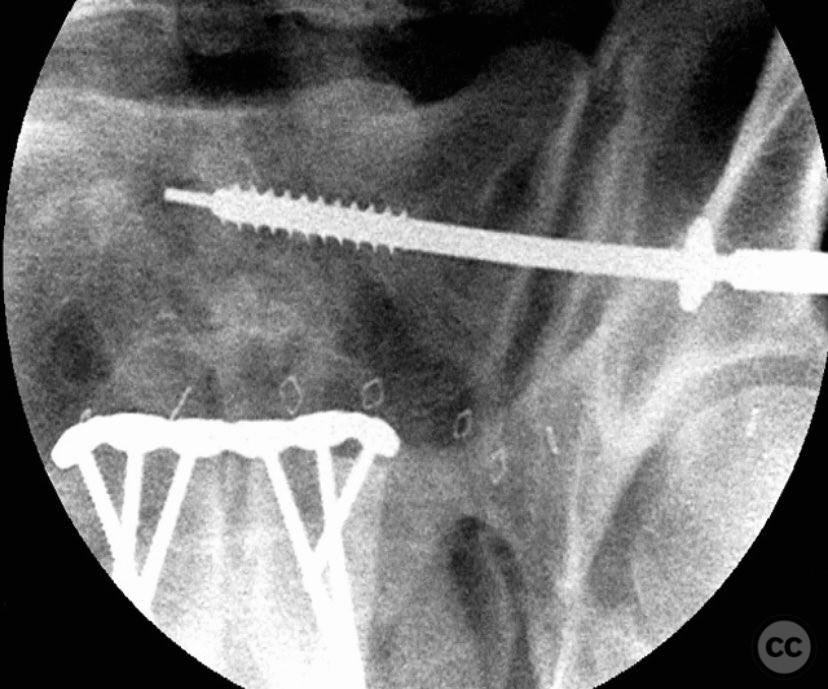
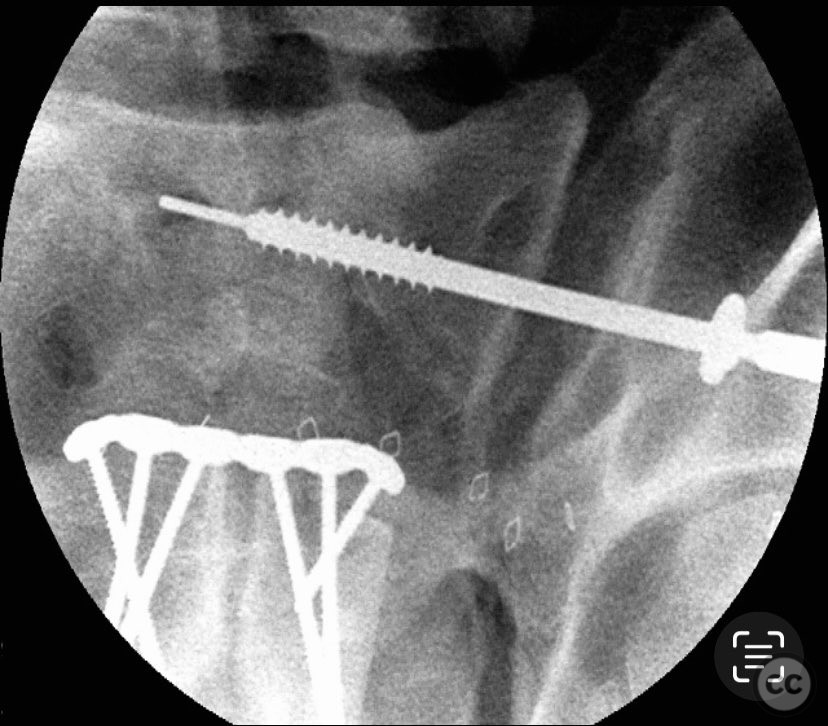
Anatomical surgical approach: A lower midline infraumbilical incision was made to expose the symphysis pubis. Subperiosteal dissection was performed to mobilize the rectus abdominis insertions and expose the pubic bodies. A pelvic reduction clamp was applied with tines docked in dense bone or soft tissue as dictated by local tissue quality, oriented to correct deformity while avoiding interference with planned plate placement. Following reduction, a contoured anterior symphyseal plate was applied and secured with cortical screws. Upon removal of the clamp, persistent SI joint malreduction was noted. Under fluoroscopic guidance, a percutaneous pathway was prepared for a cannulated iliosacral lag screw, traversing the posterior ilium into the upper sacral segment, ensuring safe passage relative to neurovascular structures.
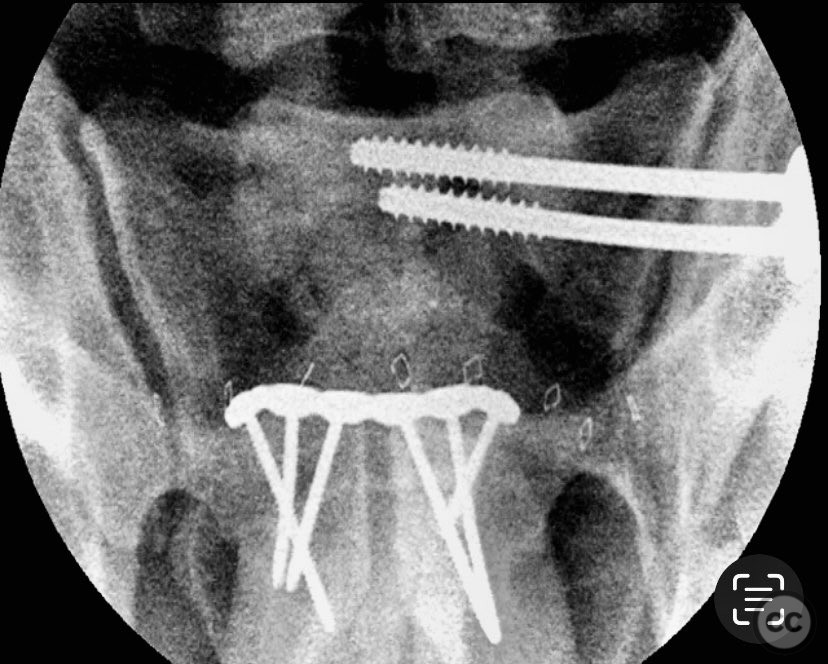
Operative remarks:The intraoperative course revealed that indirect reduction of the incomplete SI joint injury via anterior stabilization was insufficient, necessitating direct percutaneous fixation. A single cannulated iliosacral oblique lag screw was inserted under fluoroscopic control, achieving reduction, compression, and stabilization of the SI joint. Surgeon-specific technical consideration included avoidance of large-diameter drills for the posterior ilium due to limited bone stock (approximately 3 cm of ilium available for purchase), and the preference for an appropriately sized washer to optimize compression without risking iatrogenic fracture.
Postoperative protocol: Postoperatively, protected weight bearing was instituted for 6 weeks with progression to full weight bearing as tolerated thereafter. Early range of motion exercises for the hip and knee were encouraged. No external immobilization was utilized.
Follow up: Not specified
Orthopaedic implants used: 3.5 mm anterior symphyseal plate with cortical screws; 7.0 mm cannulated iliosacral lag screw with washer
Search for Related Literature


Industry Sponsership
contact us for advertising opportunities
Article viewed 293 times
11 Sep 2025
Add to Bookmarks
Full Citation
Cite this article:
Routt, ML. (2025). Combined Symphysis Pubis Disruption and Incomplete Left Sacroiliac Joint Injury in an Adult. Journal of Orthopaedic Surgery and Traumatology. Case Report 13919347 Published Online Sep 11 2025.