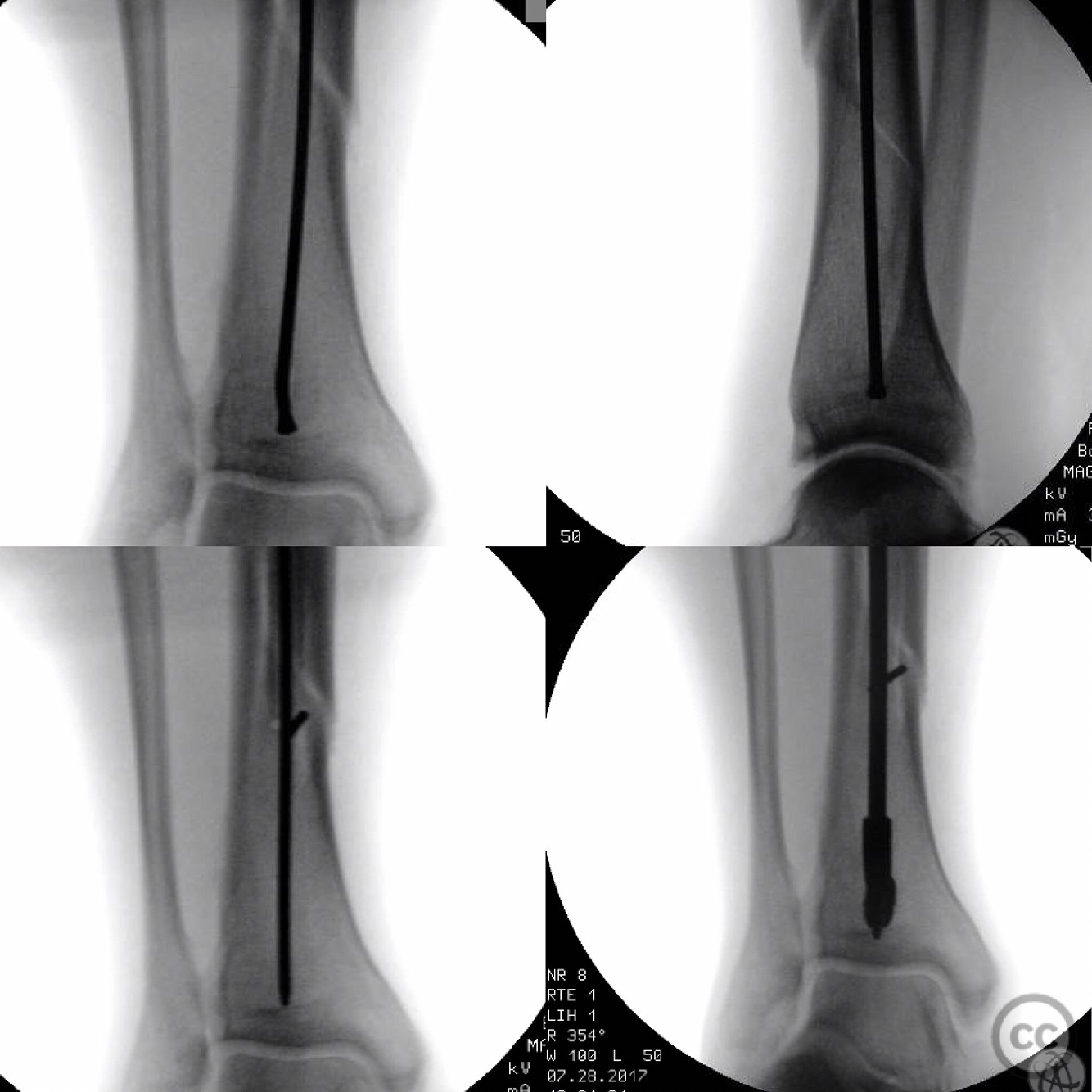
 🚘💥🏍_._._._Segmentally comminuted tibia fracture. Closed_ no evidence of compartment syndrome. ._(.jpg)
Intramedullary Nailing of Comminuted Tibial Shaft Fracture with Blocking Wire Technique.
Score and Comment on this Case
Clinical Details
Clinical and radiological findings: The patient presented with a comminuted tibial shaft fracture. Radiological assessment revealed a fracture pattern consistent with AO/OTA classification 42-C2, indicating a multifragmentary fracture of the diaphysis. The guidewire trajectory showed a tendency to deviate towards the deficient medial cortex, posing a risk for eccentric reaming and potential malreduction.
Preoperative Plan
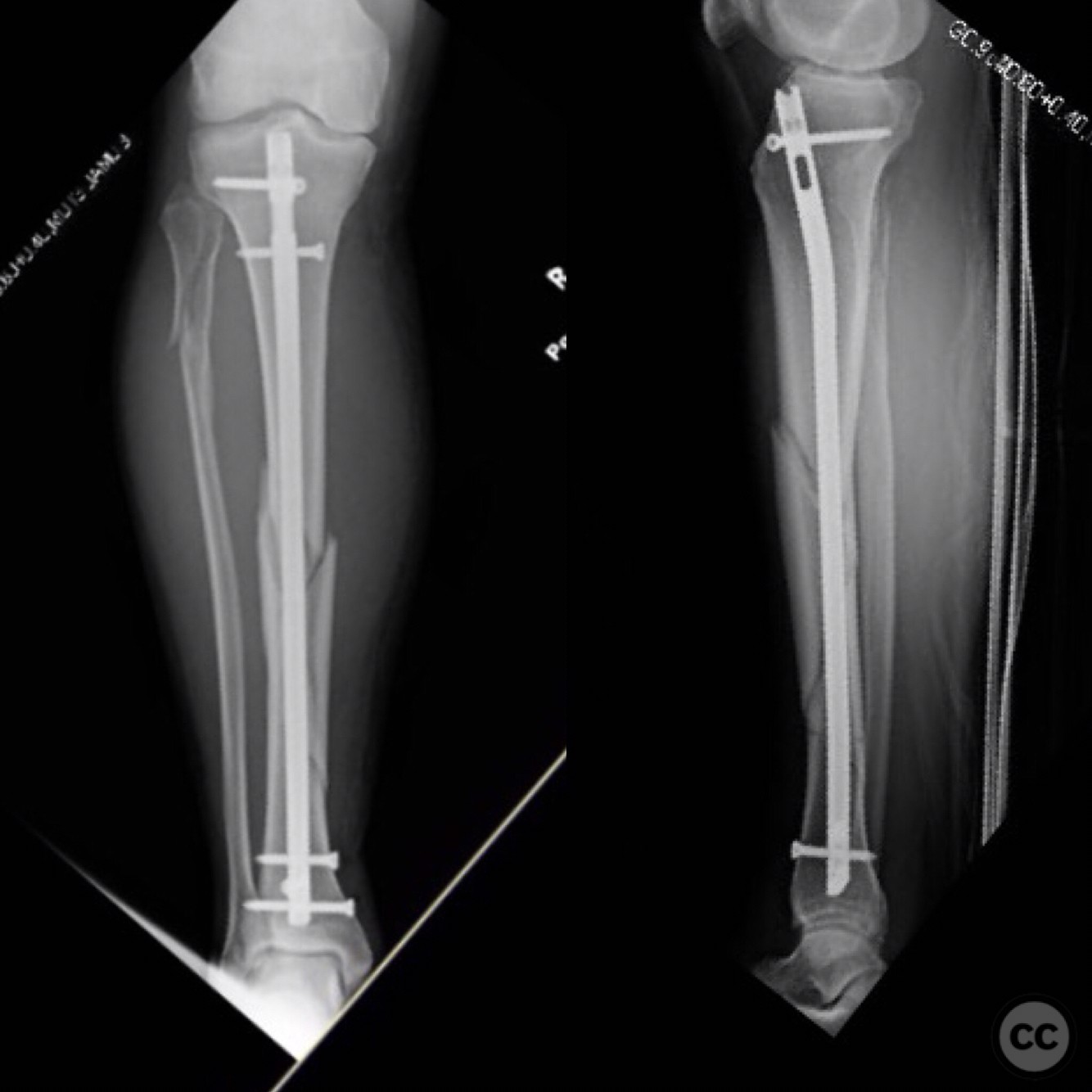
Planning remarks: The preoperative plan involved the use of an intramedullary nail for stabilization. A blocking wire was planned to control the guidewire and reamers, preventing deviation towards the deficient cortex. The surgical approach was to be through a standard infrapatellar incision for tibial nailing.
Surgical Discussion
Patient positioning: The patient was positioned supine on the operating table. A radiolucent table was used to facilitate intraoperative imaging. The knee was maintained in a semi-extended position to allow for optimal access and alignment during nailing.
Anatomical surgical approach: A longitudinal infrapatellar incision was made, followed by careful dissection to expose the proximal tibia. The entry point for the intramedullary nail was established at the anterior aspect of the tibial plateau, just medial to the lateral tibial spine. A blocking wire was placed to guide the reamers and maintain alignment.
Operative remarks:Intraoperative challenges included maintaining guidewire alignment due to the comminuted nature of the fracture. The use of a blocking wire proved essential in preventing medial deviation during reaming, ensuring proper alignment of the intramedullary nail. The semi-extended position facilitated easier access and visualization of the entry point.
Postoperative protocol: Postoperatively, the patient was advised to begin partial weight-bearing as tolerated with crutches, progressing to full weight-bearing over 6-8 weeks based on clinical and radiographic assessment. Range of motion exercises for the knee were initiated early to prevent stiffness.
Follow up: Not specified.
Orthopaedic implants used: Intramedullary nail, blocking wire, guidewire, reamers.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 317 times
25 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Intramedullary Nailing of Comminuted Tibial Shaft Fracture with Blocking Wire Technique.. Journal of Orthopaedic Surgery and Traumatology. Case Report 13669199 Published Online Jul 25 2025.