 med studs and junior residents- 1) what is the diagnosis_ 2) how are you going to(.jpg)
 med studs and junior residents- 1) what is the diagnosis_ 2) how are you going t_2.jpg)
 med studs and junior residents- 1) what is the diagnosis_ 2) how are you going t_1.jpg)








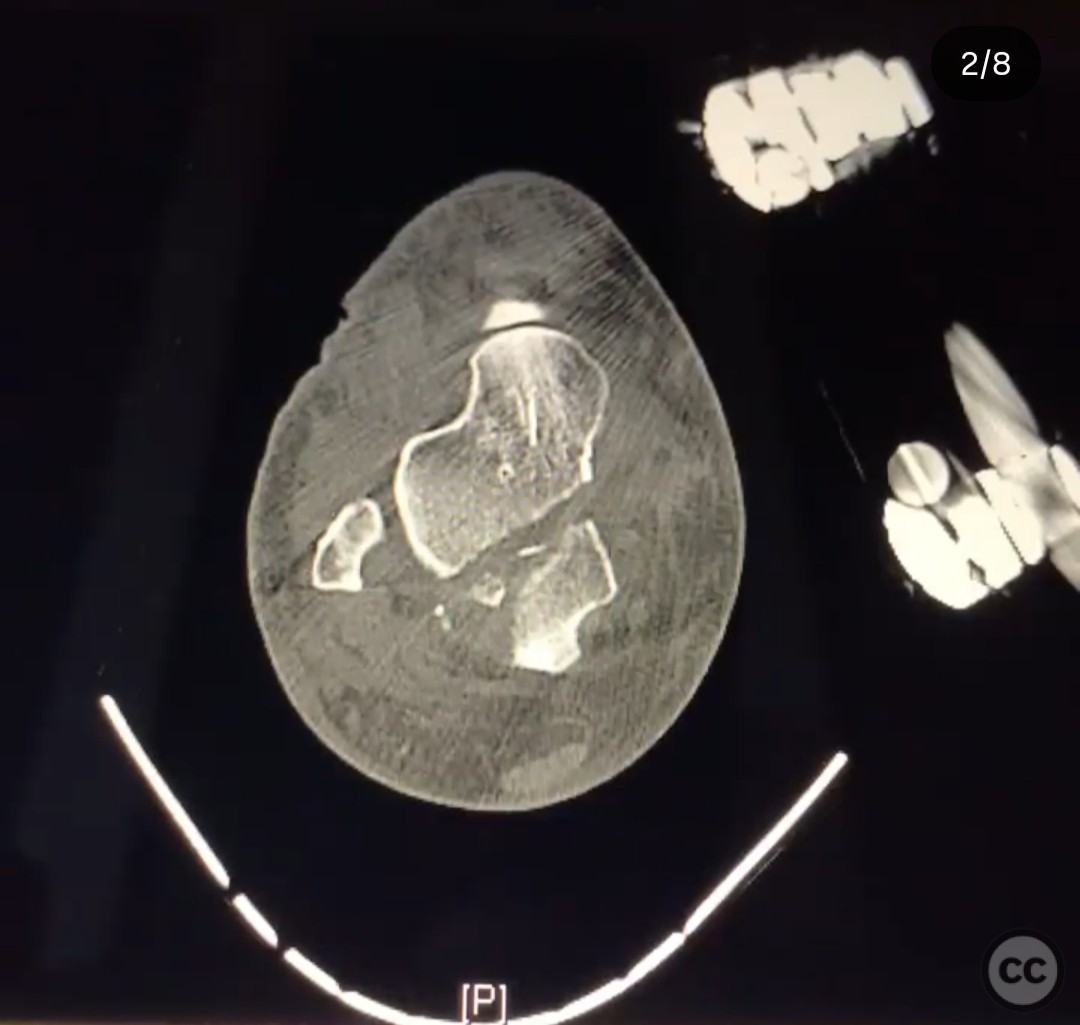







Medial Subtalar/Talonavicular Dislocation with Posterior Talar Body Fracture
Score and Comment on this Case
Clinical Details
Clinical and radiological findings: A 36-year-old female sustained a closed, isolated injury from a fall while bouldering. Initial clinical examination revealed a medial subtalar and talonavicular dislocation with a talar body fracture. Closed reduction attempts were unsuccessful due to entrapment of lateral structures, including the talonavicular capsule, extensor digitorum brevis (EDB), and extensor digitorum longus (EDL). A CT scan post-open reduction and external fixation demonstrated a displaced posterior talar body fracture and persistent subtle subtalar incongruity.
Preoperative Plan
Planning remarks: The preoperative plan involved an open reduction via a posteromedial approach to address the posterior talar body fracture. This approach was chosen to provide access to the posterior 50% of the talar dome and subtalar joint, facilitating fixation of the coronal fracture plane from posterior to anterior.
Surgical Discussion
Patient positioning: The patient was positioned prone on the operating table to allow optimal access for the posteromedial approach.
Anatomical surgical approach: A posteromedial approach was utilized, involving an incision along the medial aspect of the Achilles tendon. The flexor hallucis longus (FHL) tendon was identified and retracted. A distractor was employed to enhance visualization of the subtalar joint and facilitate reduction. Care was taken to avoid injury to the neurovascular structures in the tarsal tunnel.
Operative remarks:The surgeon noted that distraction was critical for adequate visualization and reduction of the fracture. The EDL, EDB, and talonavicular capsule were successfully repositioned during open reduction. The posteromedial approach allowed for direct fixation of the coronal fracture plane. Examination of the talonavicular joint post-reduction confirmed stability, negating the need for retention of the external fixator.
Postoperative protocol: Postoperative rehabilitation included non-weight bearing for six weeks, followed by gradual weight-bearing as tolerated. Range of motion exercises were initiated early to prevent stiffness.
Follow up: Not specified
Orthopaedic implants used: External fixator, distractor
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 306 times
18 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Medial Subtalar/Talonavicular Dislocation with Posterior Talar Body Fracture. Journal of Orthopaedic Surgery and Traumatology. Case Report 13187048 Published Online Jul 18 2025.