









AO/OTA 43-C Type Pilon Fracture with Compartment Syndrome Management
Score and Comment on this Case
Clinical Details
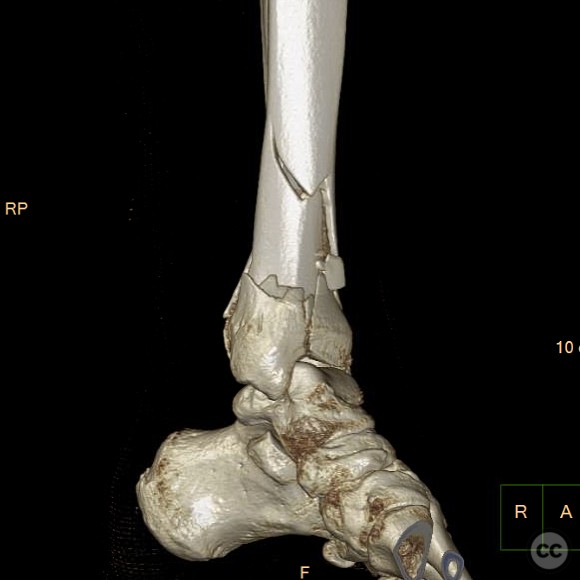
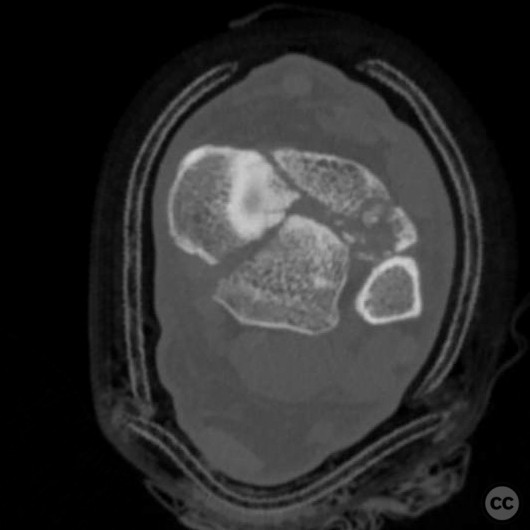
Clinical and radiological findings: A 34-year-old male sustained a fall from a height of 10 feet off a ladder, resulting in a closed C-type pilon fracture. Initial management included spanning external fixation, after which the patient developed compartment syndrome necessitating a single incision four-compartment fasciotomy. The fasciotomy wound has since been closed and is adequately healed for definitive fixation.
Preoperative Plan
Planning remarks: The preoperative plan involved an anterolateral approach to address the fracture components. The diaphyseal component was to be reduced and fixed initially, followed by disimpaction and anterior translation of the Volkmann fragment. Subsequent correction of the posteriorly translated articular block was planned, with reduction of the medial malleolar fragment using wires. Final steps included reduction of the anterior and Chaput fragments, with summative fixation using a combination of medial and anterolateral plates.
Surgical Discussion
Patient positioning: Supine positioning on the operating table was utilized, allowing for optimal access to the anterolateral aspect of the distal tibia.
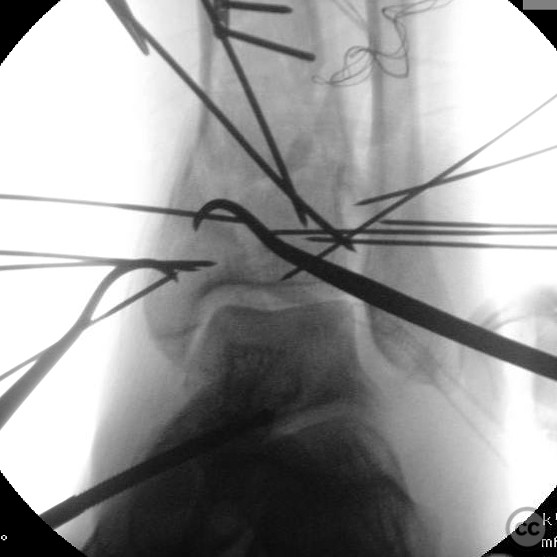
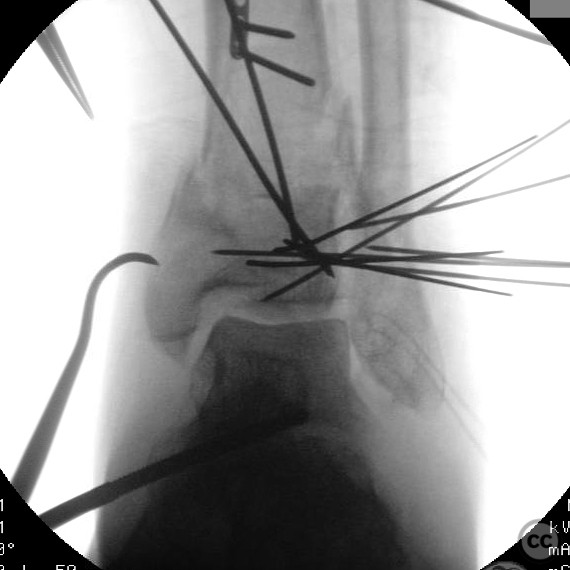
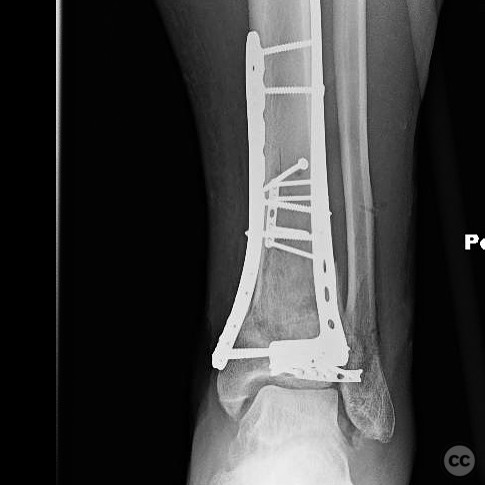
Anatomical surgical approach: A longitudinal anterolateral approach was employed, providing access to the distal tibia. Subperiosteal dissection was performed to expose the fracture site. The diaphyseal component was addressed first, followed by manipulation of the Volkmann fragment using an osteotome and hook. The articular block was then realigned, and the medial malleolar fragment was stabilized with wires. The anterior and Chaput fragments were subsequently reduced, with final fixation achieved through percutaneous application of a medial plate and an anterolateral plate.
Operative remarks:The surgeon noted that initial reduction of the diaphyseal component was achieved with a lag screw and a 2.0mm plate. The Volkmann fragment required careful disimpaction and anterior translation. Correction of the posterior translation of the articular block was crucial for alignment. The medial malleolar fragment was temporarily held with wires, while the Chaput fragment was secured with a 2.0mm hook plate. Overall, summative fixation was accomplished with a percutaneously applied medial plate and an anterolateral plate.
Postoperative protocol: Postoperative rehabilitation included non-weight bearing for six weeks, followed by gradual progression to partial weight bearing as tolerated. Range of motion exercises were initiated early to prevent stiffness.
Follow up: Not specified.
Orthopaedic implants used: Lag screw, 2.0mm plate, 2.0mm hook plate, percutaneous medial plate, anterolateral plate.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 355 times
26 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). AO/OTA 43-C Type Pilon Fracture with Compartment Syndrome Management. Journal of Orthopaedic Surgery and Traumatology. Case Report 11767009 Published Online Jul 26 2025.