














Combined Vertical Femoral Neck and Reverse Obliquity Pertrochanteric Femur Fractures in a Young Male Skier.
Score and Comment on this Case
Clinical Details
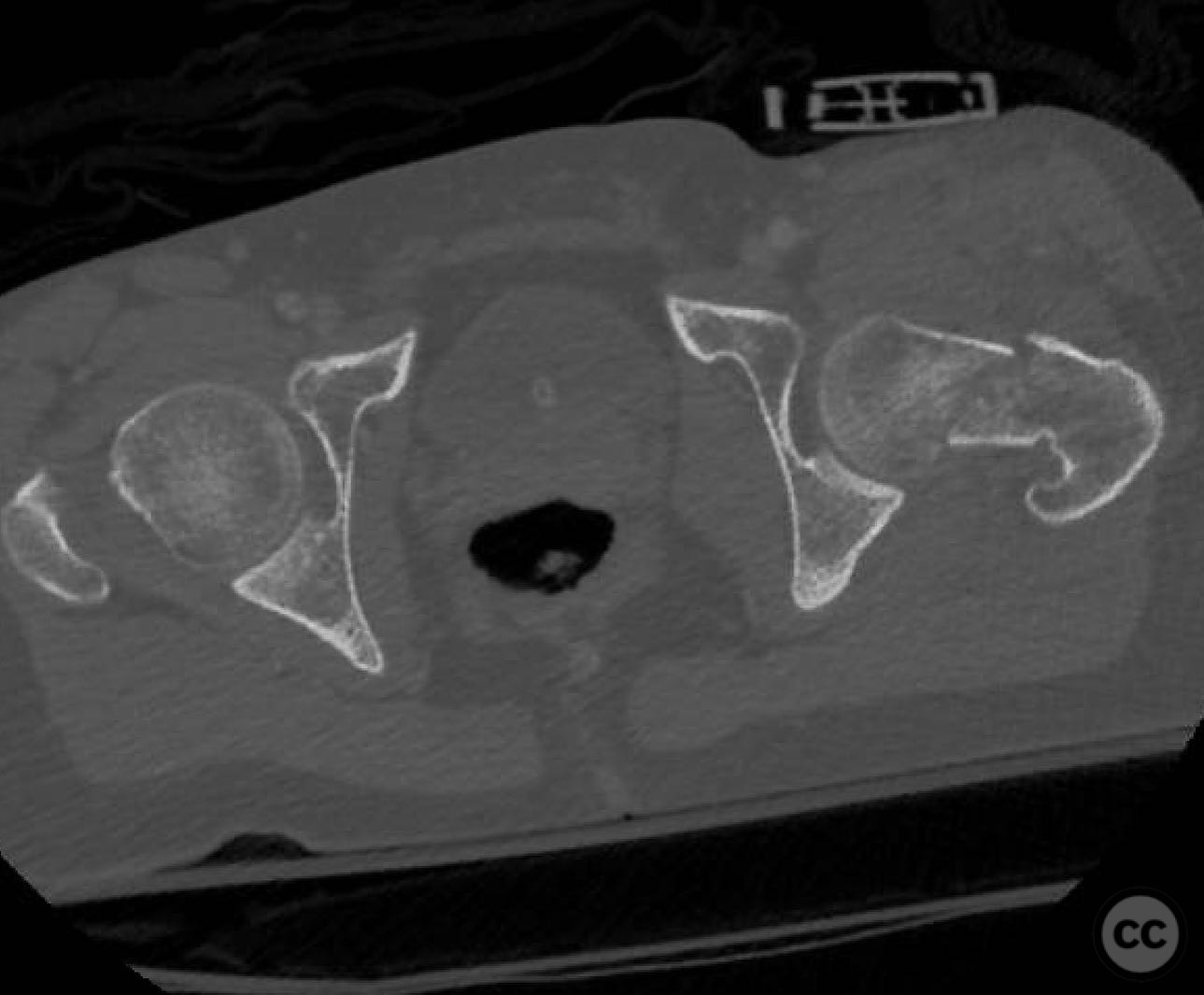
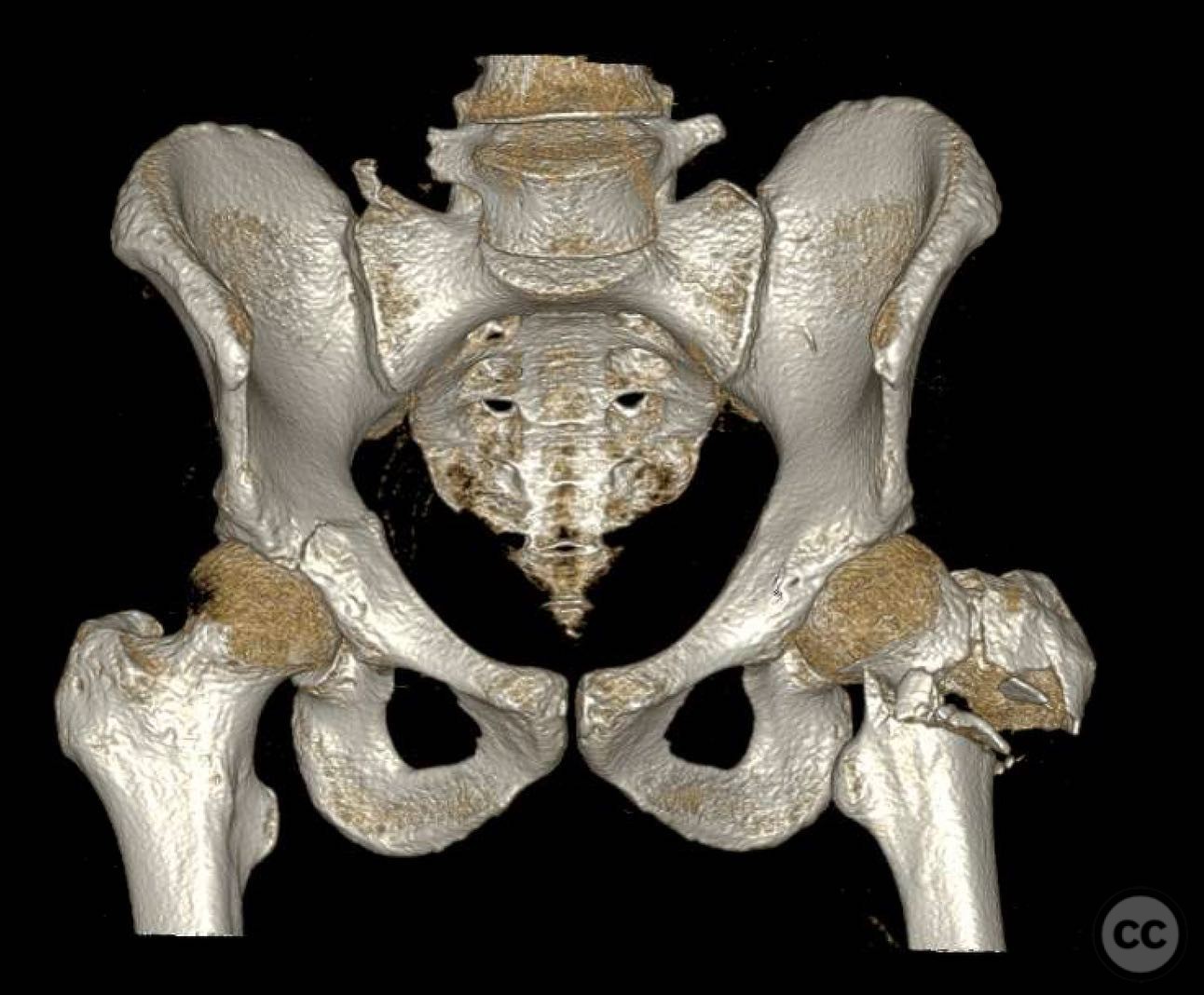
Clinical and radiological findings: A 30-year-old male sustained a high-energy skiing injury, resulting in a vertical displaced femoral neck fracture and a reverse obliquity pertrochanteric femur fracture. The patient also presented with rib fractures, hemopneumothorax, and a grade 3 kidney laceration. Radiological assessment revealed significant displacement of the femoral neck fracture and a compromised calcar region.
Preoperative Plan
Planning remarks: The preoperative plan involved an open reduction of the femoral neck fracture via a Heuter approach for optimal visualization and anatomical reduction. The pertrochanteric fracture required an anatomic reduction, with plans to use a fixed angle implant for the neck and an intramedullary nail for the reverse obliquity fracture.
Surgical Discussion
Patient positioning: The patient was positioned supine on a standard operating table, with the affected limb prepared for open reduction and internal fixation without the use of a traction table.
Anatomical surgical approach: A Heuter approach was utilized, involving an incision over the anterior aspect of the hip, allowing direct access to the femoral neck for anatomical reduction. The approach facilitated visualization and reduction of the vertical neck fracture. The pertrochanteric region was addressed through the same incision, ensuring adequate exposure for intramedullary nailing.
Operative remarks:The surgeon emphasized the complexity of achieving simultaneous reductions of both fractures. Stout wires were employed to secure the reductions, placed anteriorly and posteriorly to the anticipated nail path. Due to the absence of calcar support, a strong biocomposite material was used to fill the gap and resist varus collapse. The choice of implants was critical, with a fixed angle device for the neck and an intramedullary nail for the pertrochanteric fracture.
Postoperative protocol: Postoperative rehabilitation included non-weight bearing on the affected limb for six weeks, followed by progressive weight bearing as tolerated. Range of motion exercises were initiated early to prevent joint stiffness.
Follow up: Not specified.
Orthopaedic implants used: Fixed angle implant for femoral neck, intramedullary nail for pertrochanteric fracture, stout wires, biocomposite material.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 258 times
16 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Combined Vertical Femoral Neck and Reverse Obliquity Pertrochanteric Femur Fractures in a Young Male Skier.. Journal of Orthopaedic Surgery and Traumatology. Case Report 11170363 Published Online Jul 16 2025.