



 only by the surgeon who is doing the definitive operation_ 2)only in(.jpg)
 only by the surgeon who is doing the definitive operation_ 2)only i_1.jpg)
 only by the surgeon who is doing the definitive operation_ 2)only i_2.jpg)
 only by the surgeon who is doing the definitive operation_ 2)only i_3.jpg)
 only by the surgeon who is doing the definitive operation_ 2)only i_4.jpg)
 only by the surgeon who is doing the definitive operation_ 2)only i_5.jpg)




Staged Management of High-Energy Pilon Fracture With Early Volkmann Reduction and Conversion From AO/OTA C-Type to B-Type Configuration
Score and Comment on this Case
Clinical Details
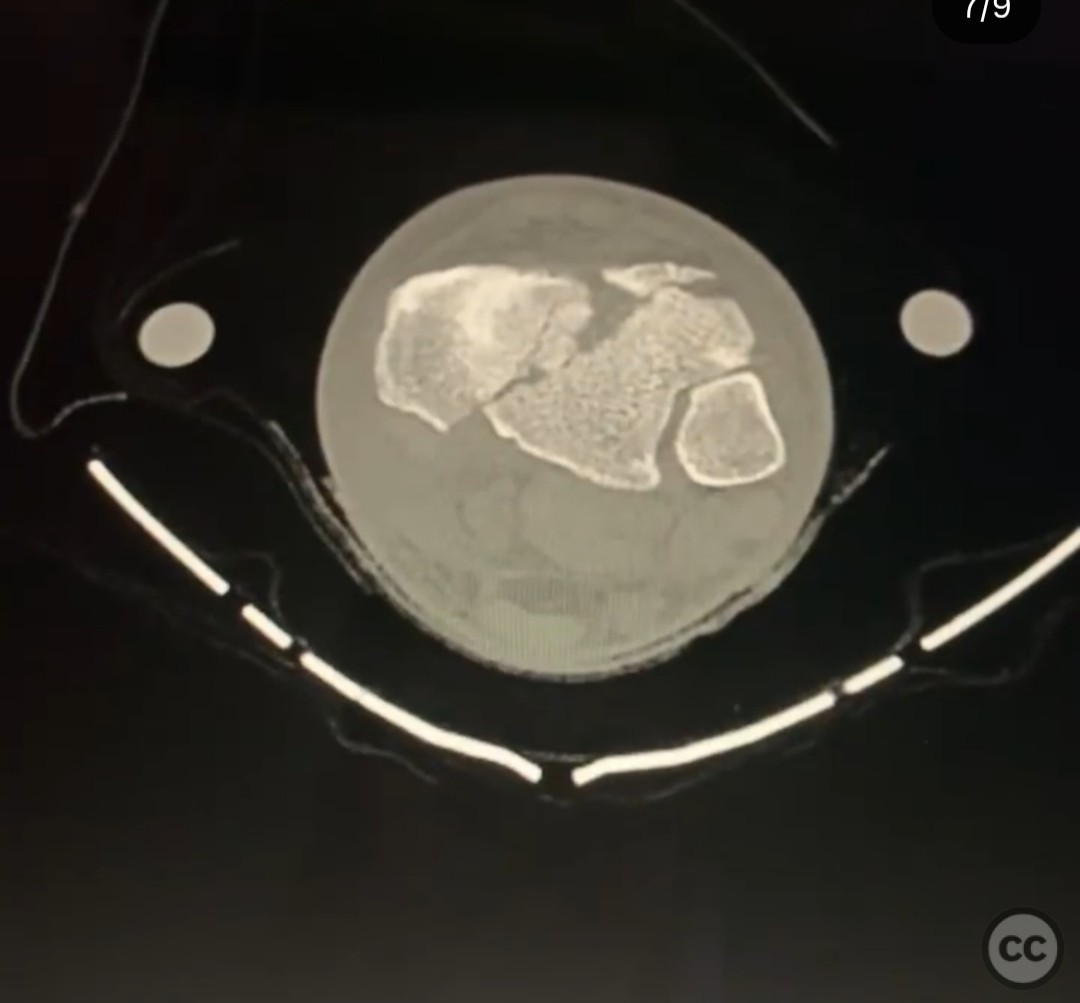
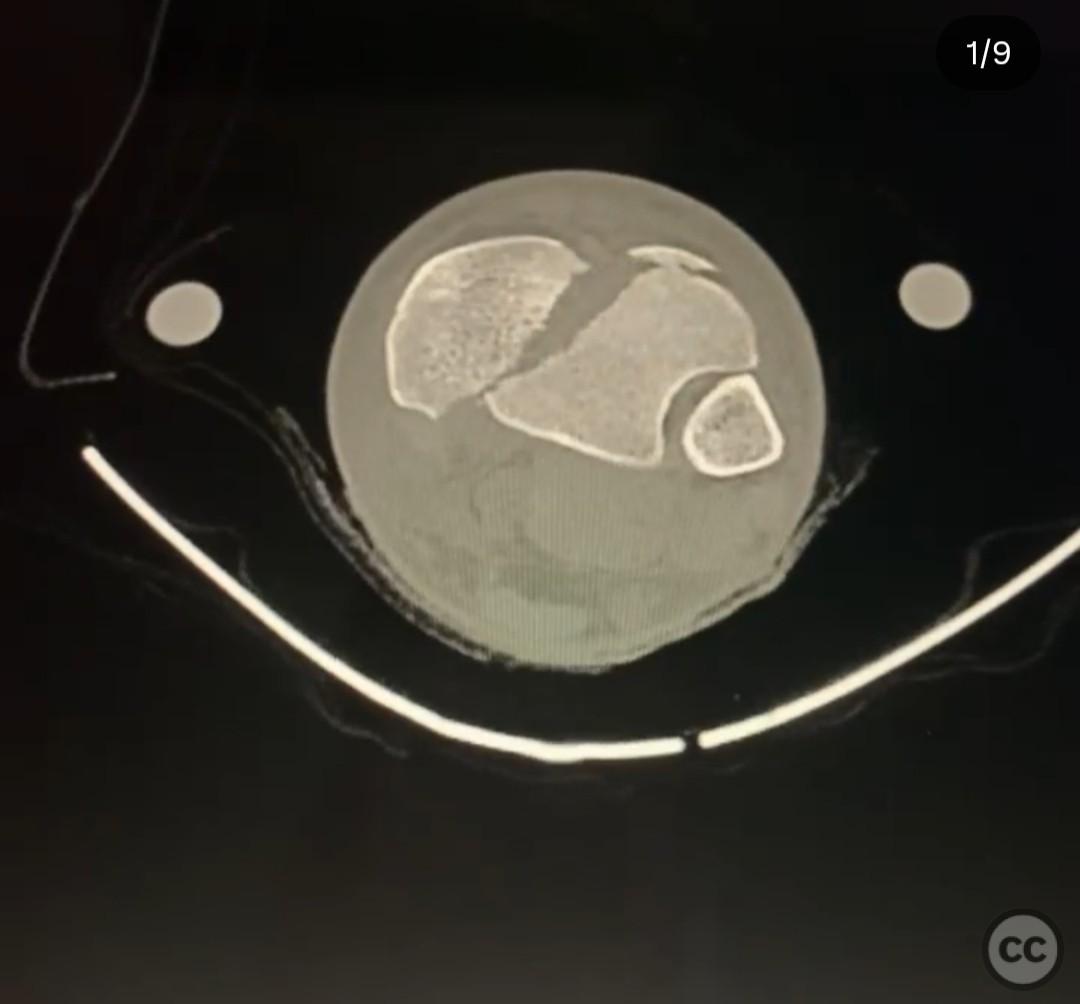
Clinical and radiological findings: A 33-year-old male sustained a closed left pilon fracture after a 20-foot fall while climbing, impacting the wall with his left foot. The injury presented with medium swelling and serous blisters anteriorly, but no vascular injury or compartment syndrome was noted. Initial radiographs and CT scan confirmed a high-energy AO/OTA 43-C3 fracture pattern with varus failure, marginal impaction in the Volkmann and medial fragment, and intercalary articular comminution.
Preoperative Plan
Planning remarks: The preoperative plan involved a staged approach. Stage 1 included external fixation to restore length, alignment, and rotation (LAR) and allow soft tissue recovery. The fracture was converted from a C-type to a B-type using a limited posteromedial approach with antiglide plating of the Volkmann fragment. A subsequent CT scan was planned for detailed surgical planning of definitive fixation.
Surgical Discussion
Patient positioning: Supine position with the affected limb elevated and prepared for both posteromedial and anteromedial surgical approaches.
Anatomical surgical approach: The initial surgical approach was a limited posteromedial incision to access the Volkmann fragment for antiglide plating. In the definitive fixation stage, an anteromedial approach was utilized to address the joint access, allowing disimpaction of marginal impaction in the Volkmann and medial fragments using osteotomes, followed by backfilling with allograft. The intercalary articular comminution was addressed through this approach.
Operative remarks:The surgeon noted the importance of converting the fracture from a C-type to a B-type early to facilitate easier reduction and stabilization, thereby improving the effectiveness of the external fixator in maintaining LAR. The primary implant was placed medially to resist varus failure, and care was taken to remove any posterior syndesmotic fragments.
Postoperative protocol: Postoperative rehabilitation included non-weight bearing with progressive weight-bearing as tolerated, contingent on radiographic evidence of healing and soft tissue recovery.
Follow up: Not specified.
Orthopaedic implants used: External fixator, antiglide plate, osteotomes, allograft material.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 344 times
18 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Staged Management of High-Energy Pilon Fracture With Early Volkmann Reduction and Conversion From AO/OTA C-Type to B-Type Configuration. Journal of Orthopaedic Surgery and Traumatology. Case Report 11098743 Published Online Jul 18 2025.