













Complex Humerus Nonunion with Radial and Musculocutaneous Nerve Deficits
Score and Comment on this Case
Clinical Details
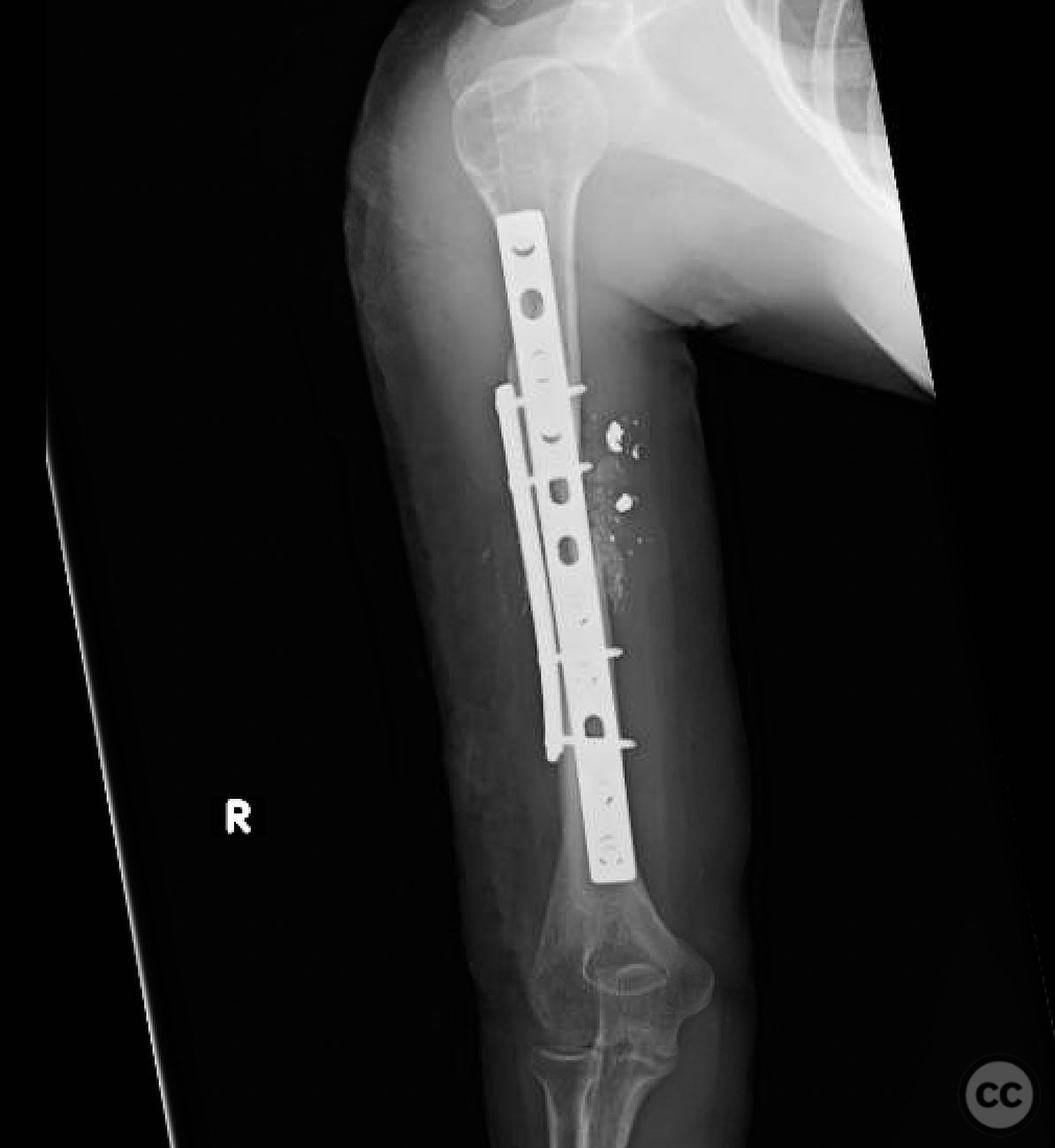
Clinical and radiological findings: A young female patient presented with a nonunion of the humerus following a gunshot wound. Initial treatment at an outside hospital included a lengthening nail and radial nerve grafting, which was unsuccessful. The patient also exhibited musculocutaneous nerve dysfunction. Radiological evaluation revealed a segmental defect and a broken distal interlock of the nail. Nonunion laboratory tests were normal, indicating no infection.
Preoperative Plan
Planning remarks: The preoperative plan involved removal of the existing nail, neurolysis of the radial nerve, and structural support using a fibula strut graft. Additional bone grafting from the iliac crest was planned, combining corticocancellous and cancellous grafts. Double plating was considered for stabilization.
Surgical Discussion
Patient positioning: The patient was positioned supine on the operating table with the affected arm placed on a radiolucent arm board to allow for optimal access and imaging.
Anatomical surgical approach: A modified Gerwin approach was utilized, involving a posterior incision along the lateral border of the triceps brachii muscle. The radial nerve was carefully identified and neurolysed. The humeral shaft was exposed subperiosteally for grafting and plating.
Operative remarks:Intraoperatively, a painful radial nerve neurolysis was performed due to significant scar tissue. A fibula strut graft was placed within the defect for structural support, supplemented by iliac crest bone grafts with osteogenic properties. Double plating was employed to ensure robust fixation and stability of the nonunion site.
Postoperative protocol: Postoperative rehabilitation included immobilization in a functional brace, with gradual range of motion exercises initiated at 2 weeks post-surgery. Weight-bearing activities were restricted until radiographic evidence of union was observed.
Follow up: Not specified
Orthopaedic implants used: Fibula strut graft, iliac crest bone graft, double plating system.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 339 times
16 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Complex Humerus Nonunion with Radial and Musculocutaneous Nerve Deficits. Journal of Orthopaedic Surgery and Traumatology. Case Report 11059875 Published Online Jul 16 2025.