

_ ._._._This is a motorcyclist with a 3b open tibia and segmental bone loss. Options for treatment of segmental bone loss include 1_3.jpg)
_ ._._._This is a motorcyclist with a 3b open tibia and segmental bone loss. Options for treatment of segmental bone loss include 1_2.jpg)
_ ._._._This is a motorcyclist with a 3b open tibia and segmental bone loss. Options for treatment of segmental bone loss include 1_1.jpg)
_ ._._._This is a motorcyclist with a 3b open tibia and segmental bone loss. Options for treatment of segmental bone loss include 1_4.jpg)


_ ._._._This is a motorcyclist with a 3b open tibia and segmental bone loss. Options for treatment of segmental bone loss include 1_6.jpg)
_ ._._._This is a motorcyclist with a 3b open tibia and segmental bone loss. Options for treatment of segmental bone loss include 1_5.jpg)
Masquelet Technique for Type 3b Open Tibial Fracture with Segmental Bone Loss
Score and Comment on this Case
Clinical Details
Clinical and radiological findings: A 56-year-old male involved in a motorcycle accident sustained a type 3b open tibial fracture with segmental bone loss. Initial radiographs and clinical examination confirmed the presence of significant bone loss and soft tissue injury. The fracture was classified as AO/OTA 42-C3, indicating a complex diaphyseal fracture with comminution. The patient presented with a simple fibular fracture, which served as a guide for tibial length and rotation during reconstruction.
Preoperative Plan
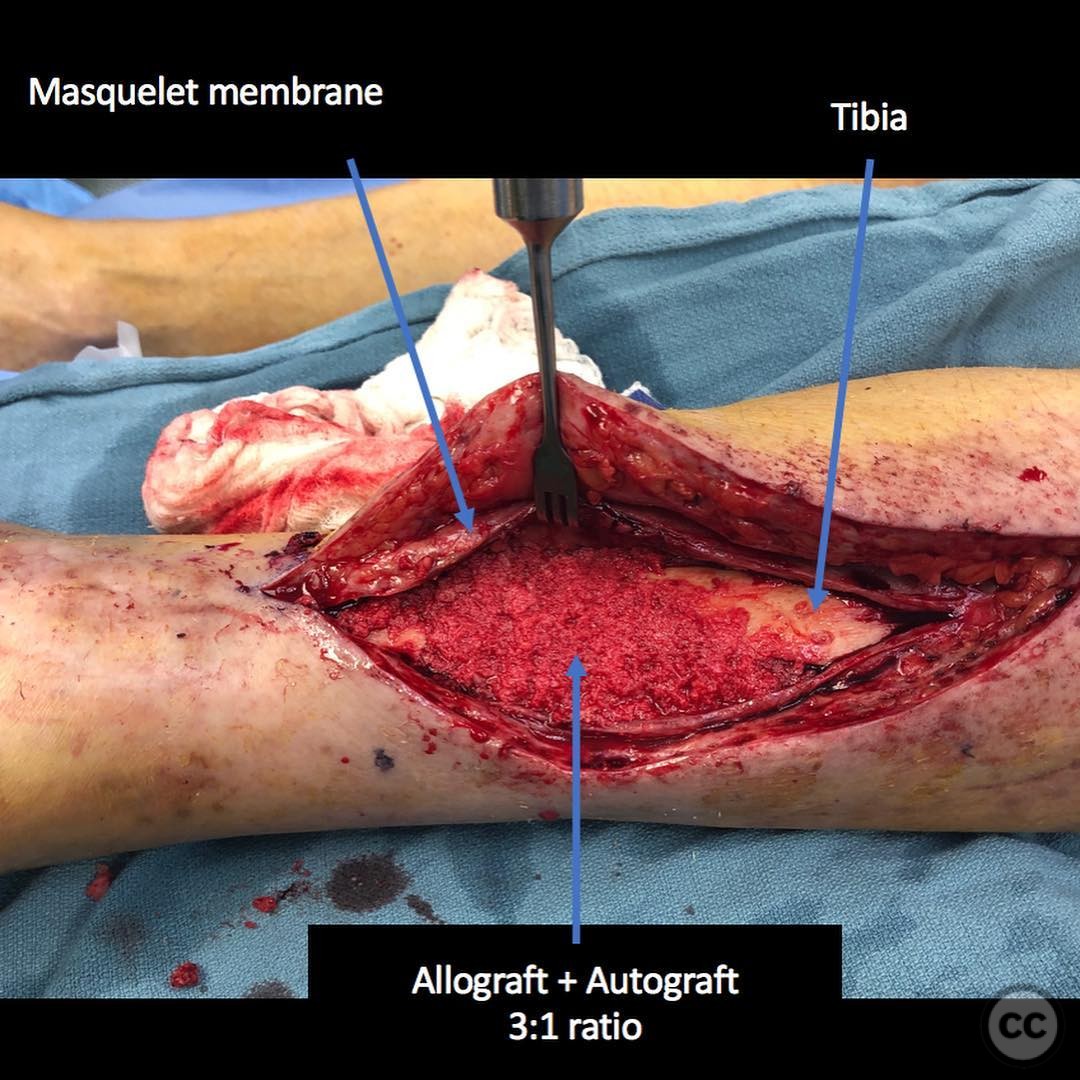
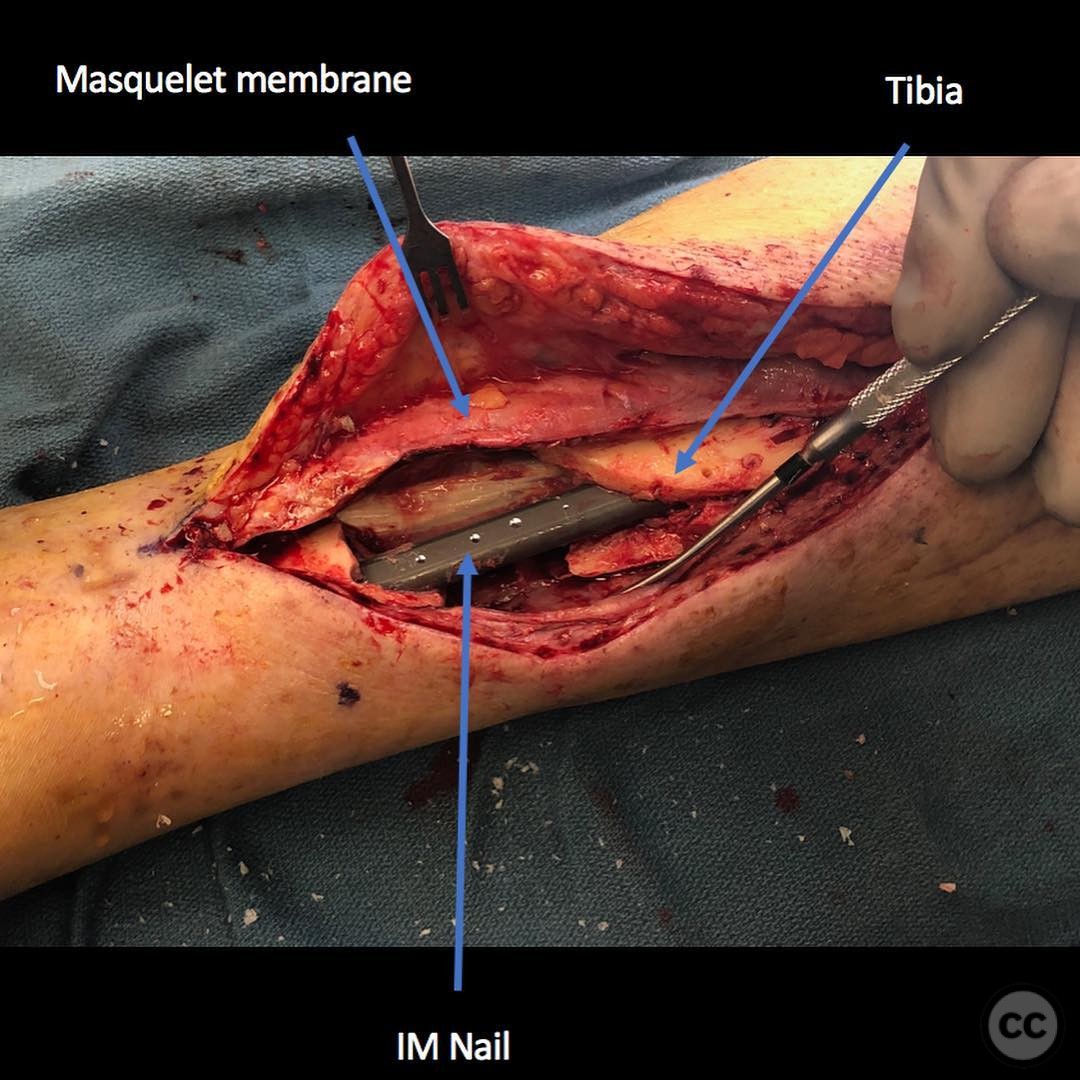
Planning remarks: The preoperative plan involved the use of the Masquelet technique. This included meticulous debridement of devitalized bone and soft tissue, followed by the placement of an intramedullary nail to stabilize the tibia and a cement spacer to fill the defect. The cement spacer was impregnated with antibiotics to prevent infection.
Surgical Discussion
Patient positioning: The patient was positioned supine on the operating table, with the affected leg prepared and draped in a sterile fashion. A tourniquet was not utilized to allow for assessment of soft tissue perfusion.
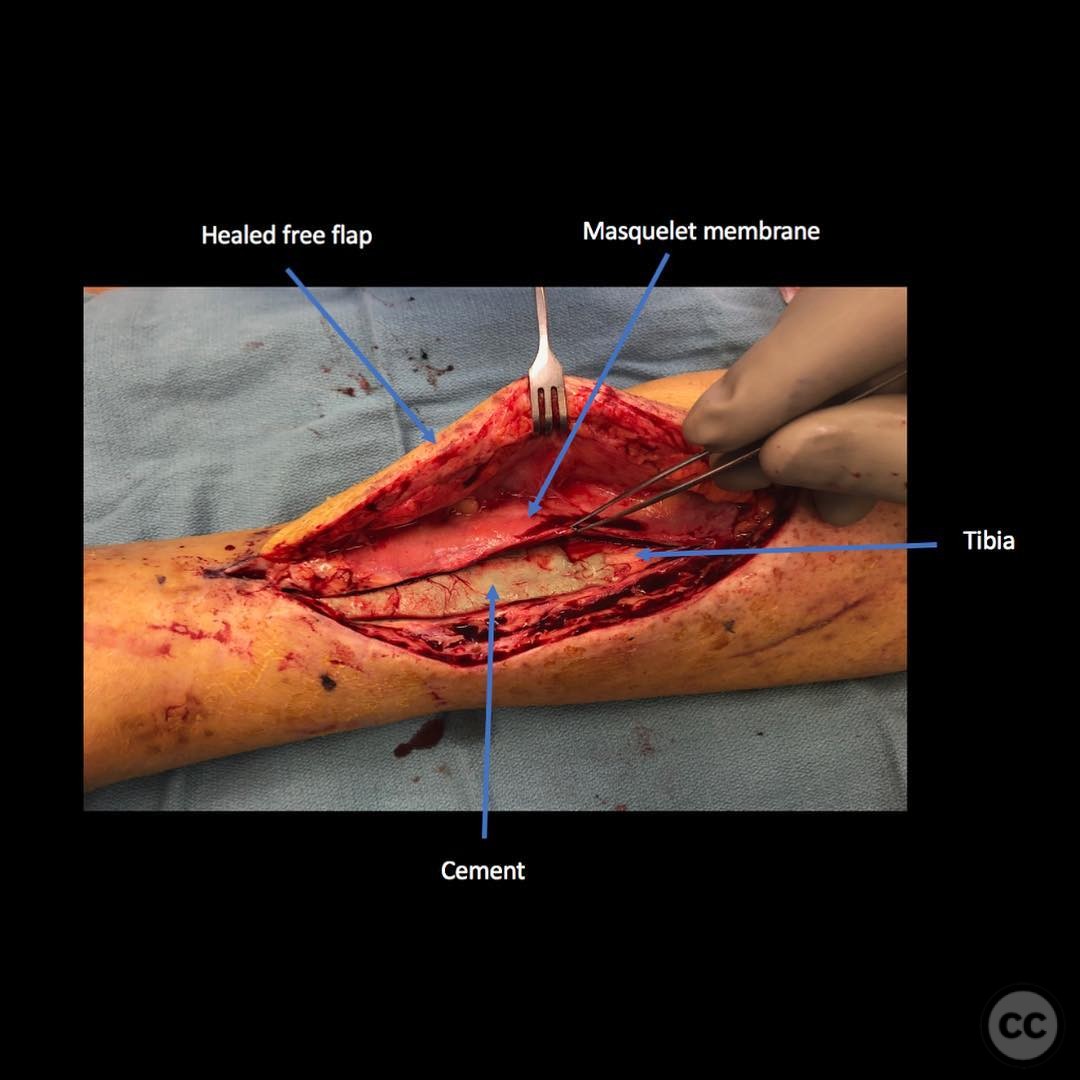
Anatomical surgical approach: A longitudinal incision was made over the anteromedial aspect of the tibia. Careful subperiosteal dissection was performed to expose the fracture site. Devitalized bone and soft tissue were meticulously debrided. An intramedullary nail was inserted for stabilization, and a cement spacer was placed within the defect, overlapping the native tibia to facilitate membrane formation.
Operative remarks:The surgeon emphasized the importance of preserving the bio-active membrane formed over the cement spacer, which is rich in osteogenic cytokines. The contralateral femur was used as a donor site for autograft harvesting via Reamer-Irrigator-Aspirator (RIA) technique, which was then expanded with allograft. The bone graft was carefully laid into the defect without excessive packing, and the membrane was closed over the graft to promote osteogenesis.
Postoperative protocol: Postoperatively, the patient was placed in a splint with non-weight bearing status on the affected limb. Early range of motion exercises were encouraged for adjacent joints, with gradual progression to weight-bearing as tolerated following confirmation of graft incorporation.
Follow up: Not specified.
Orthopaedic implants used: Intramedullary nail, antibiotic-impregnated cement spacer, RIA system for autograft harvesting.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 281 times
21 Jul 2025
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2025). Masquelet Technique for Type 3b Open Tibial Fracture with Segmental Bone Loss. Journal of Orthopaedic Surgery and Traumatology. Case Report 11049155 Published Online Jul 21 2025.