




Transverse with Comminuted Posterior Wall Acetabular Fracture-Dislocation Treated by Prone Kocher-Langenbeck Approach
Score and Comment on this Case
Clinical Details
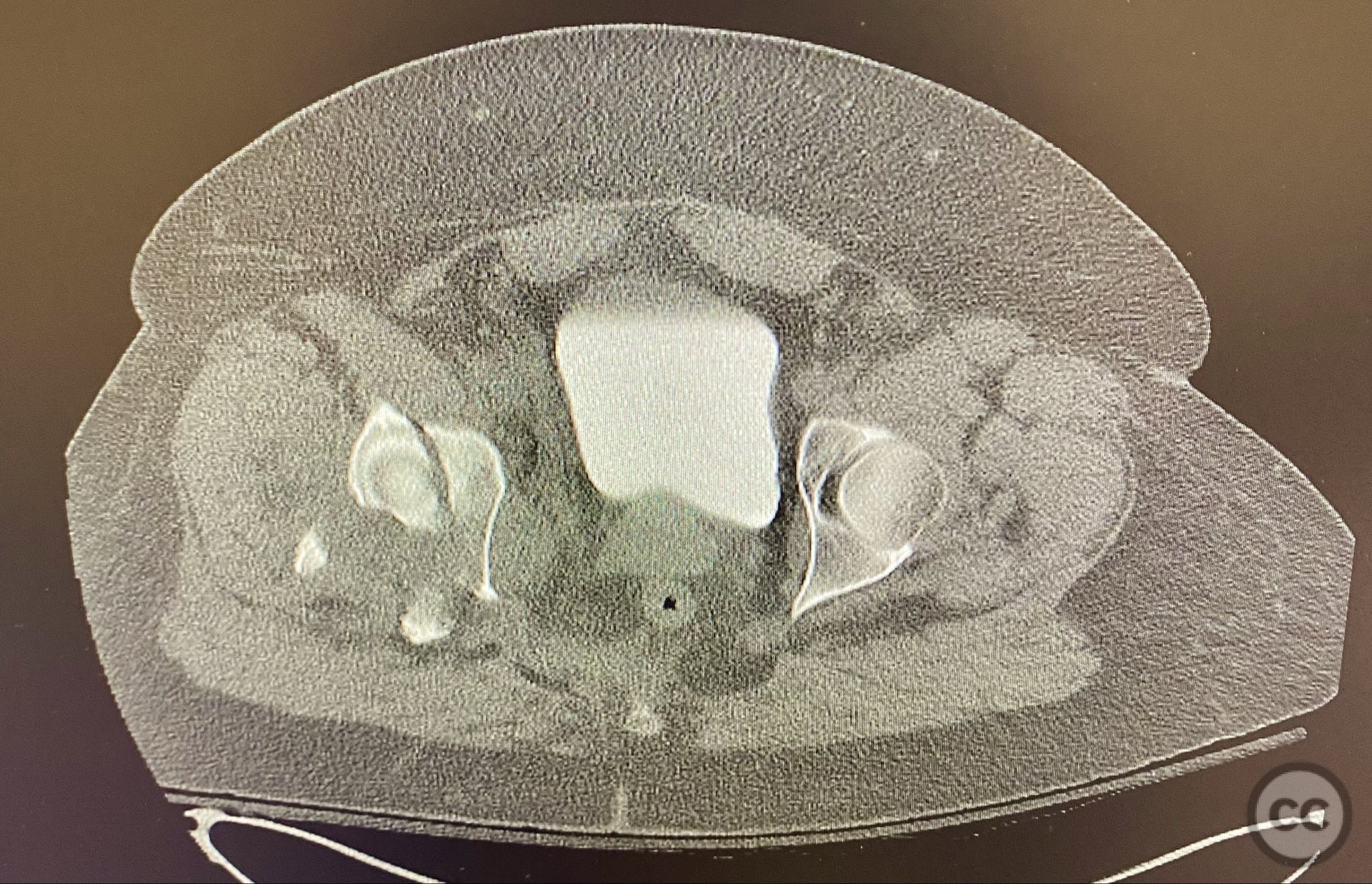
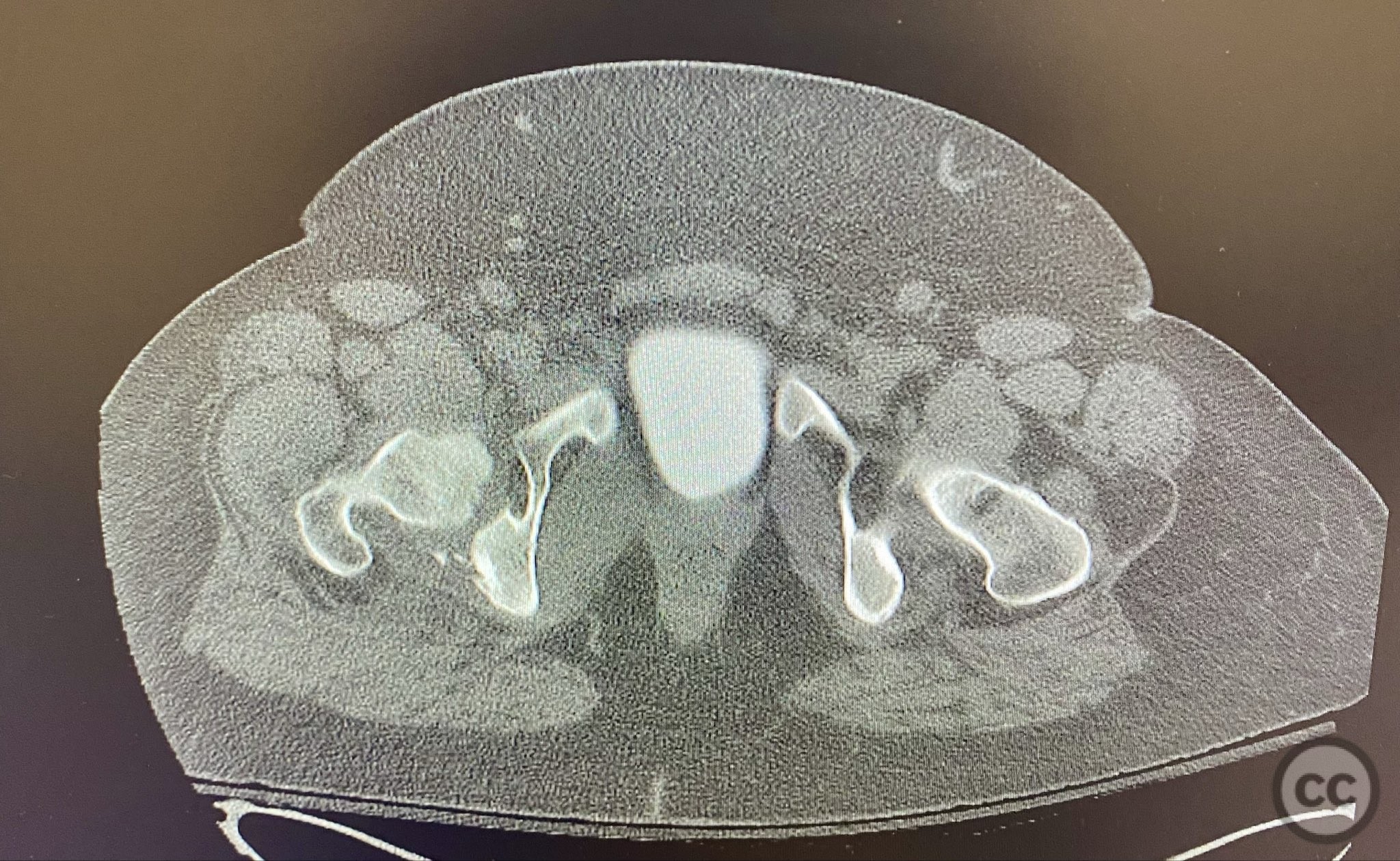
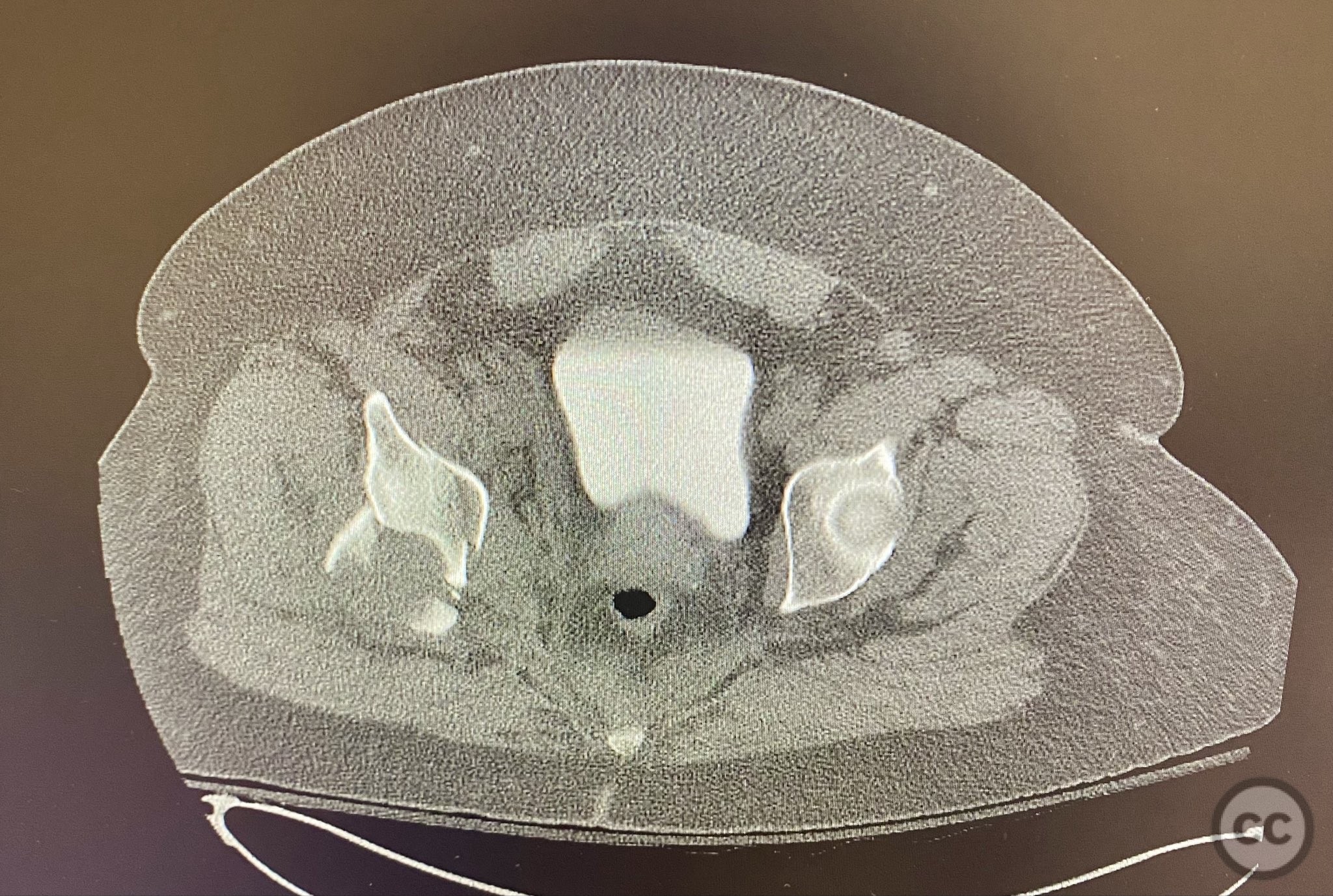
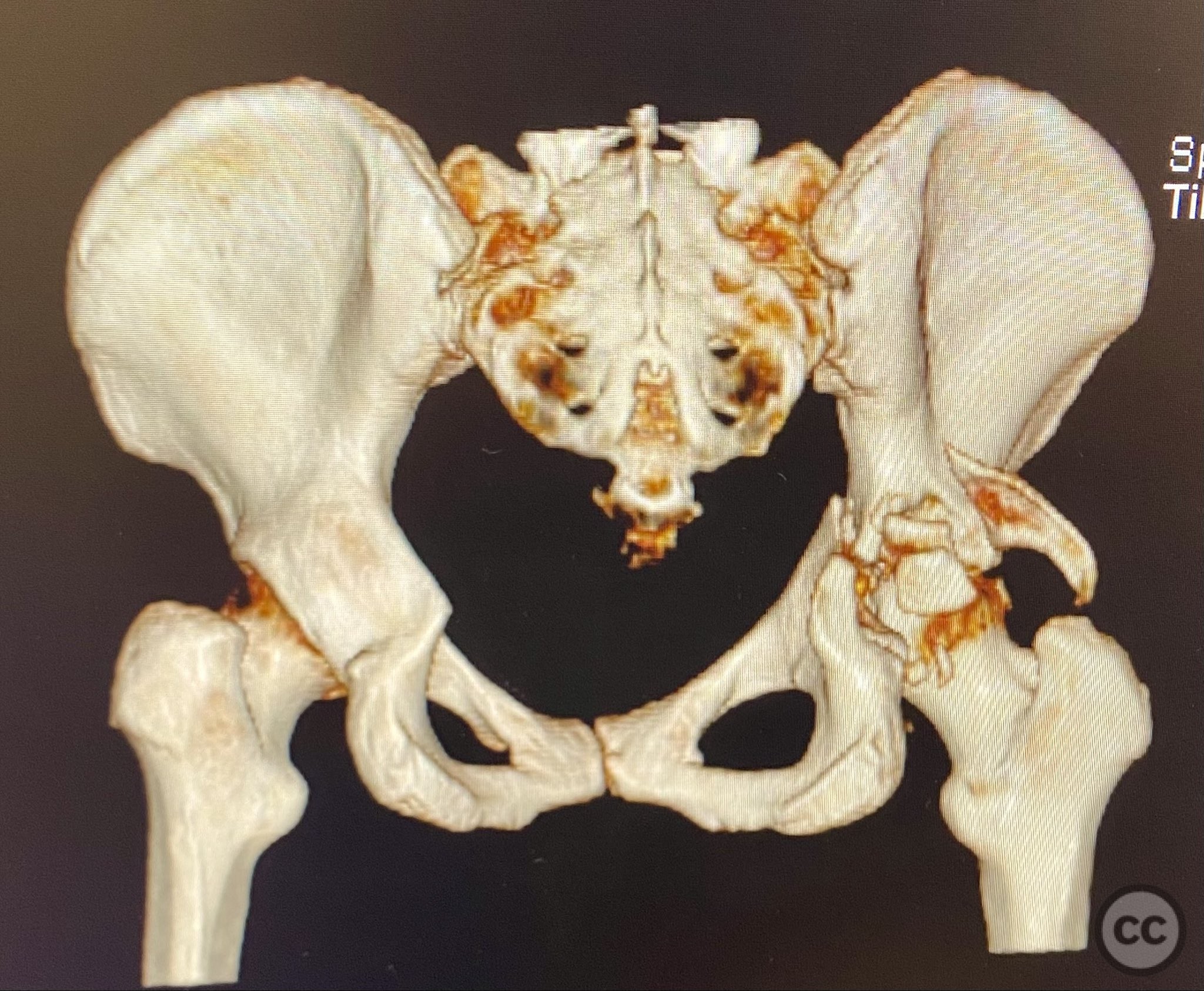
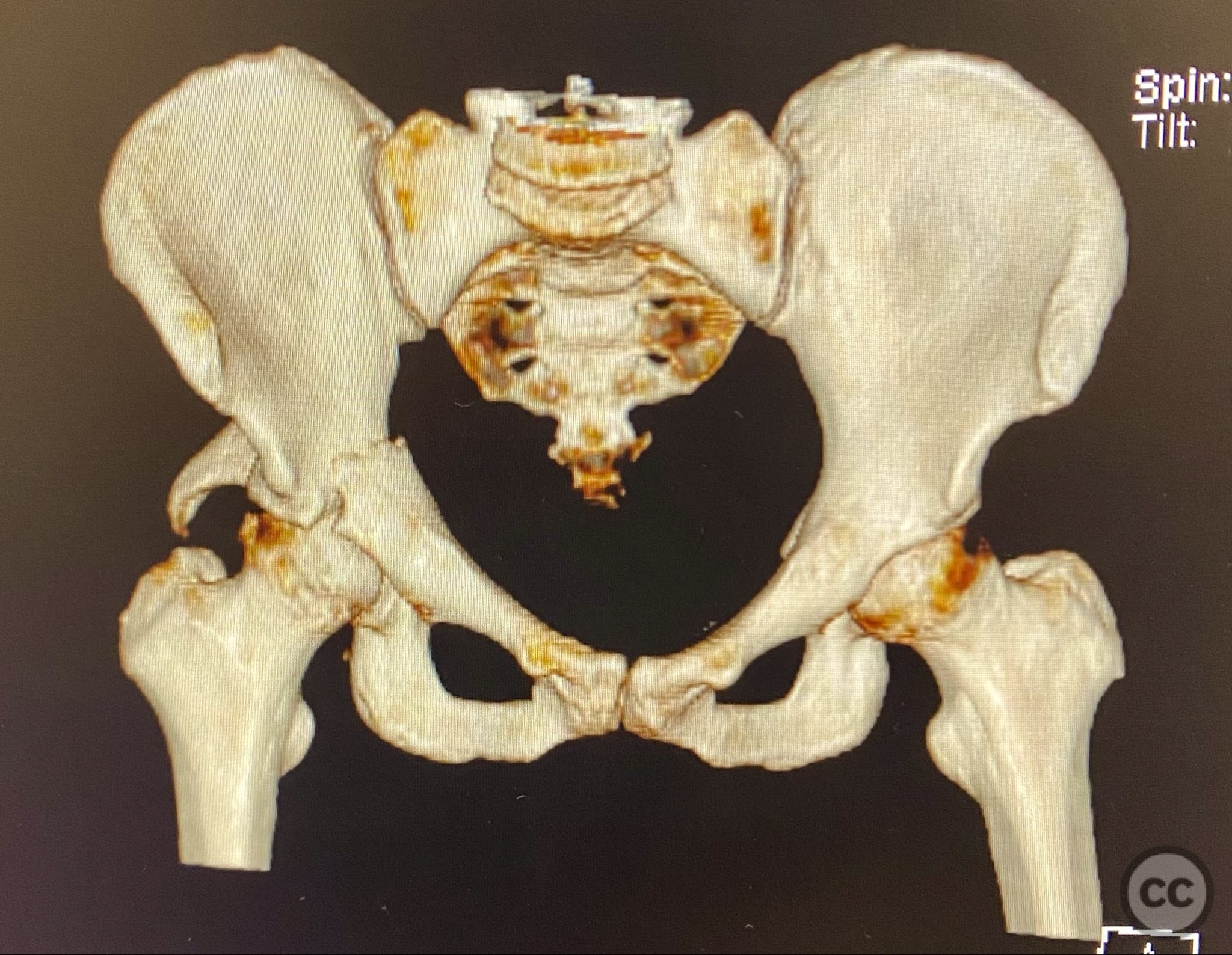
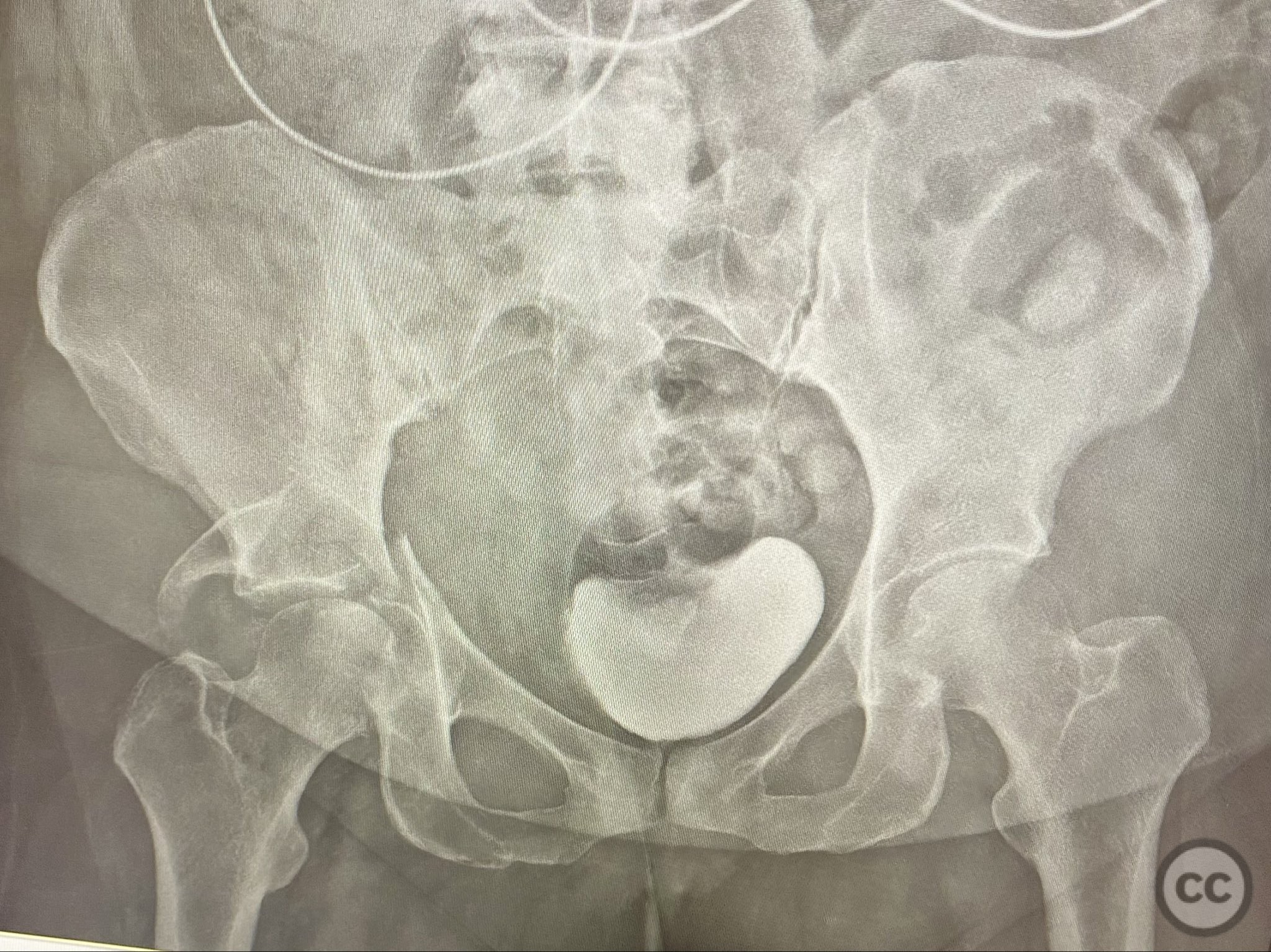
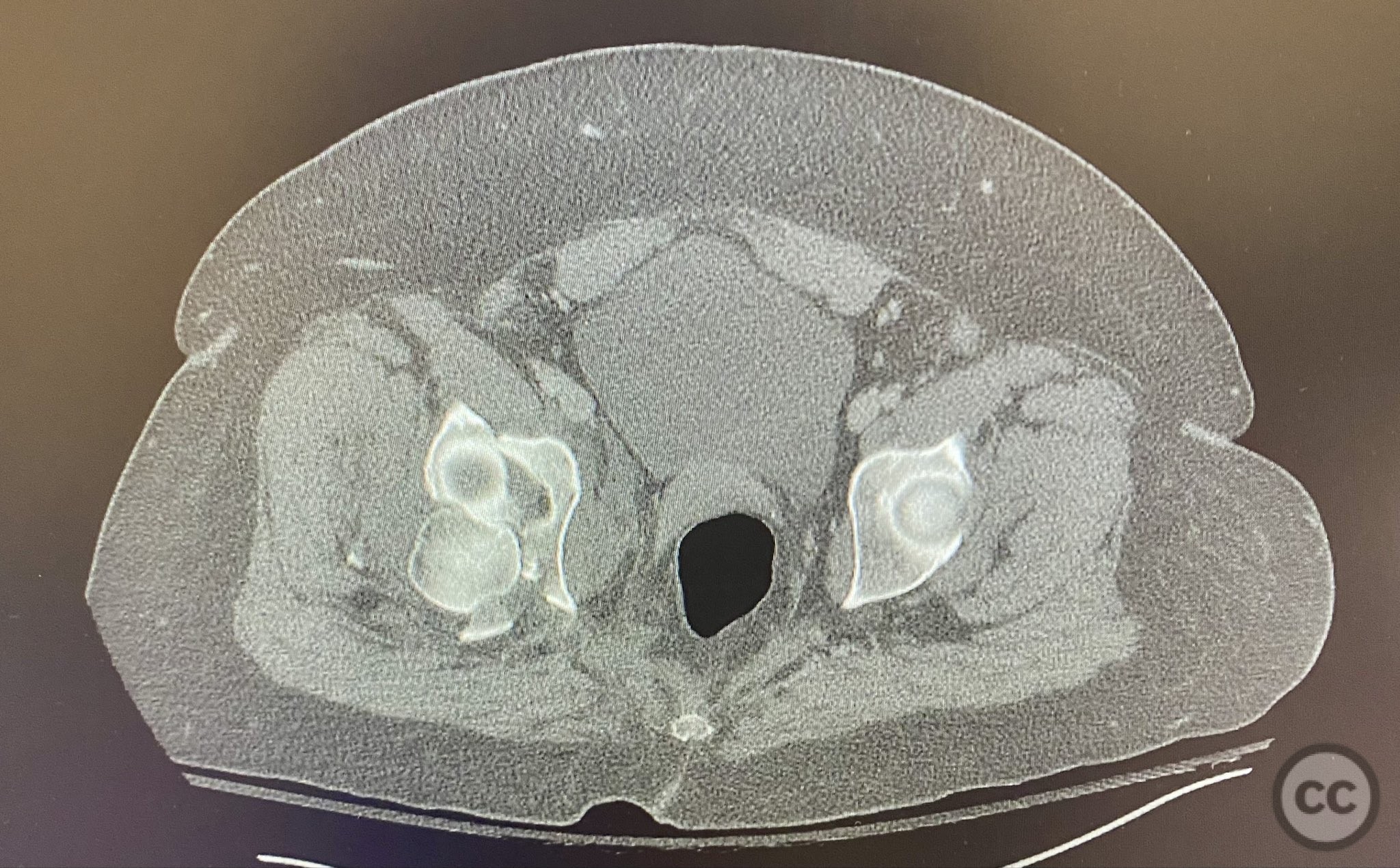
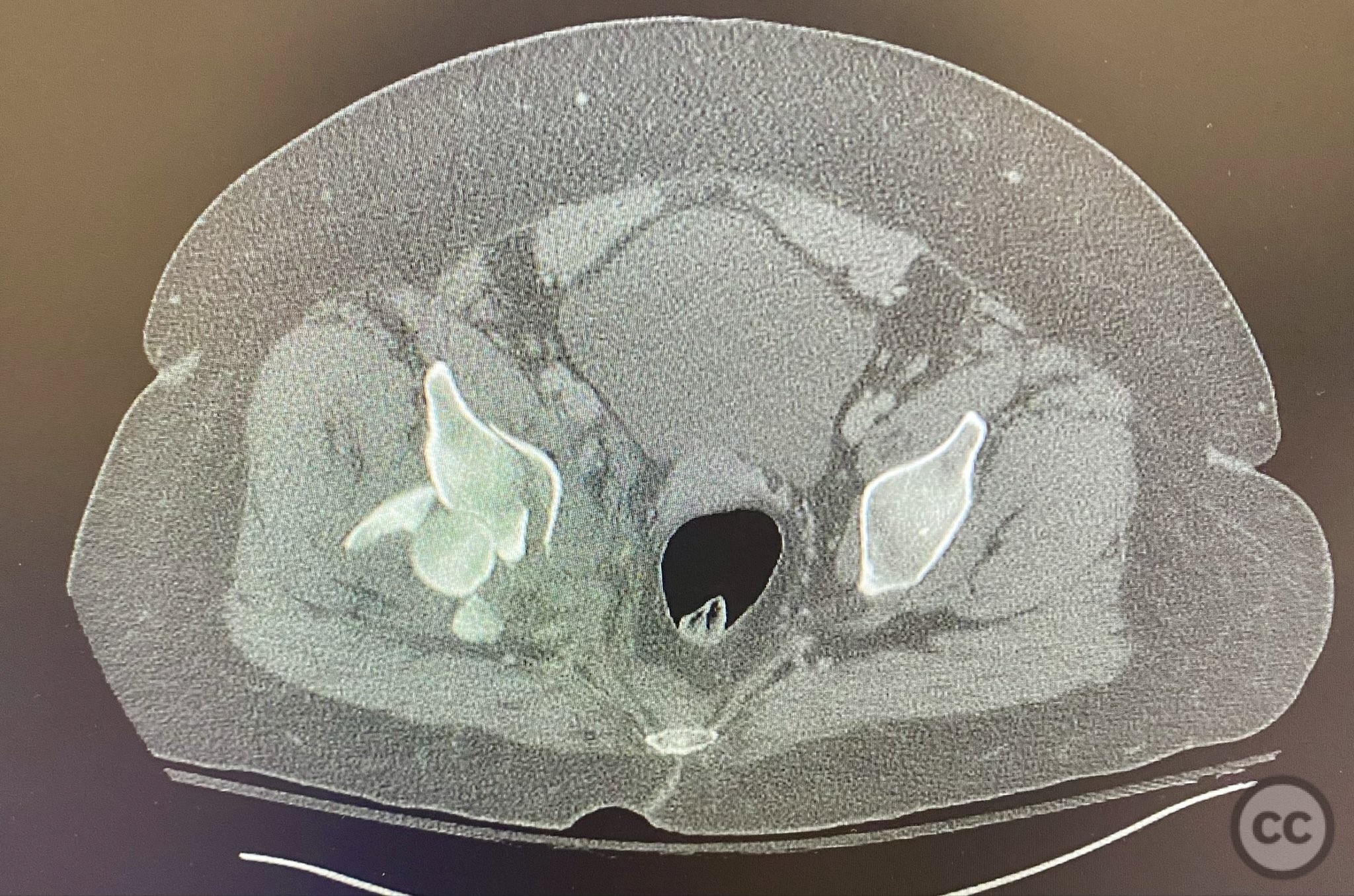
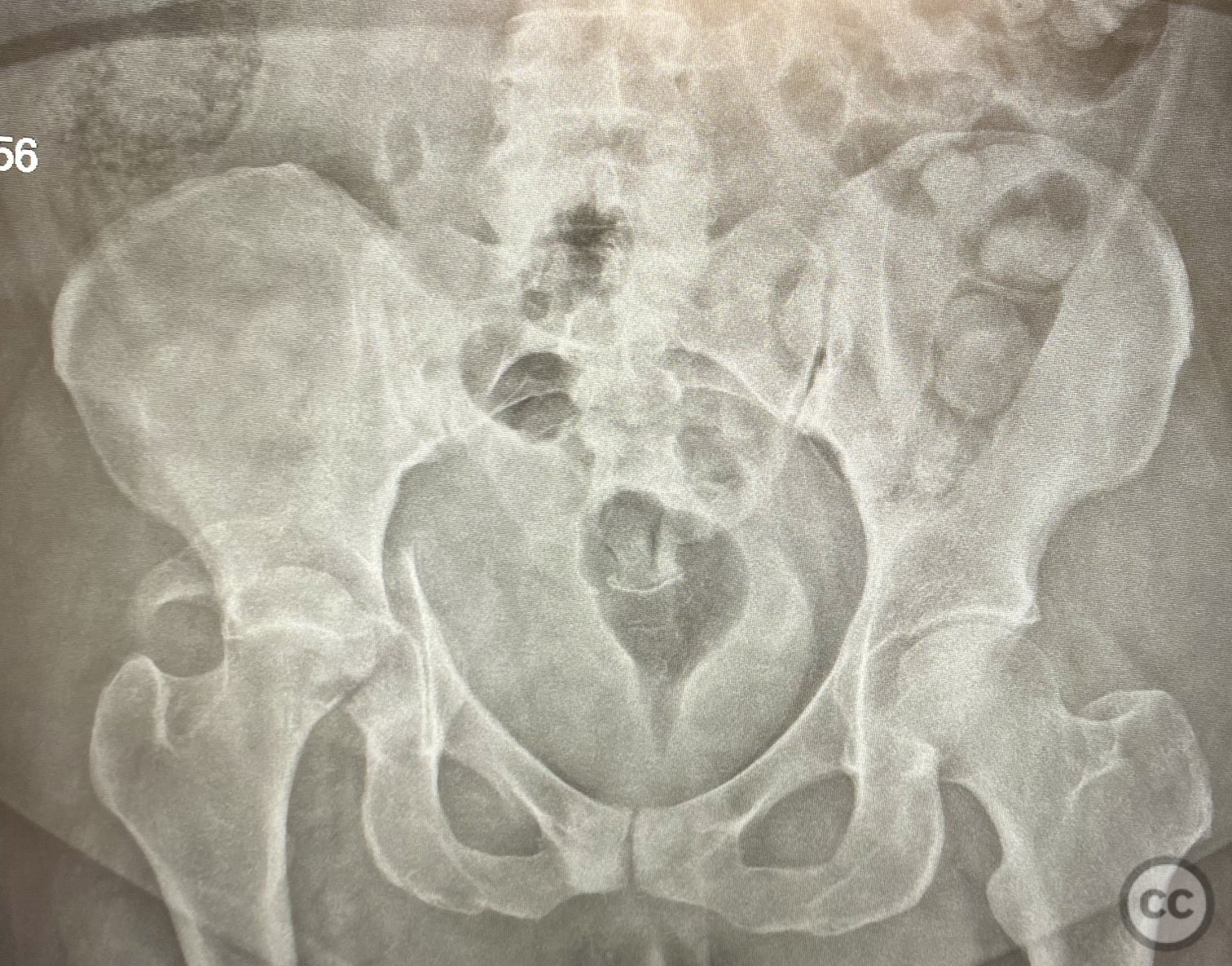
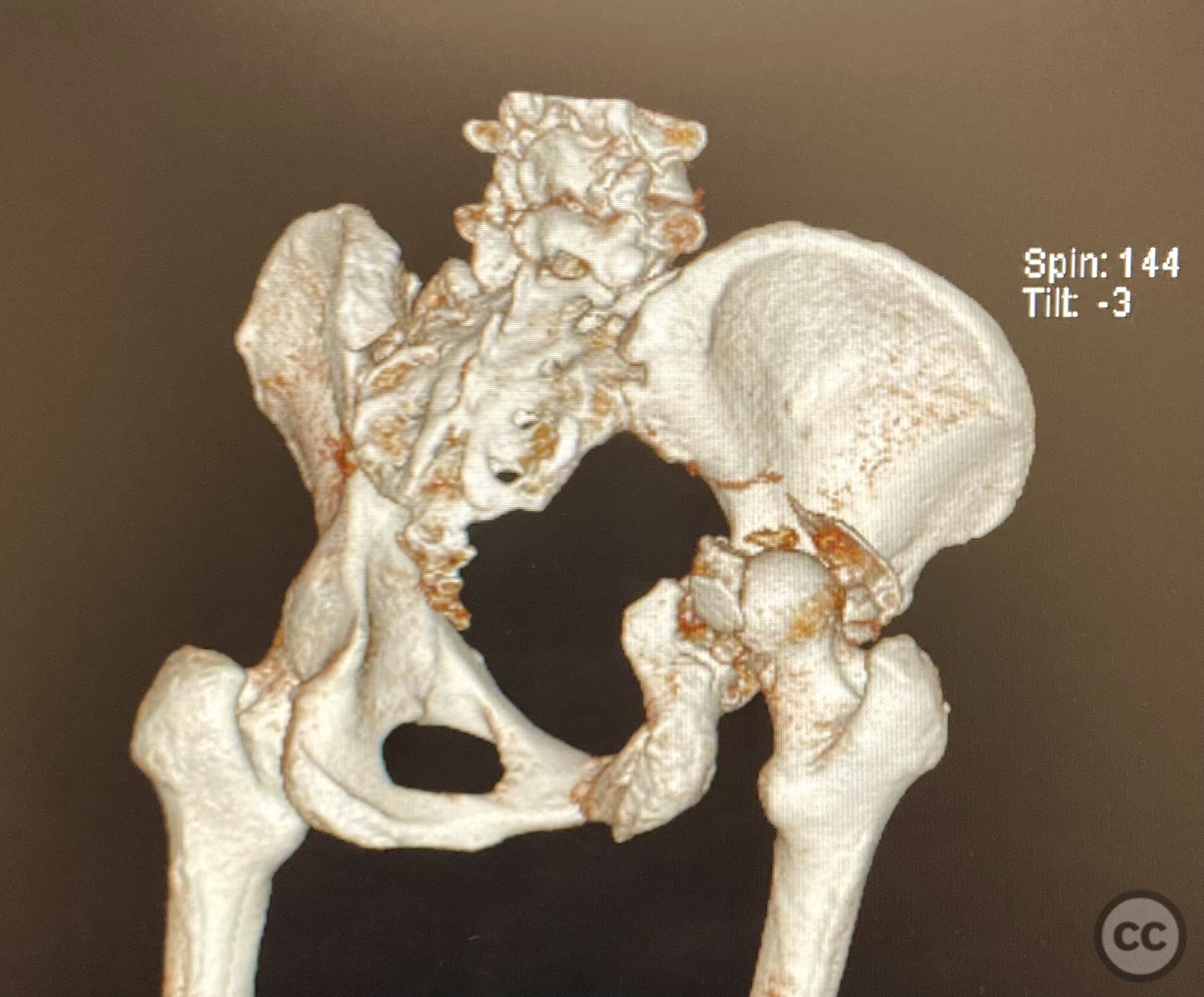
Clinical and radiological findings: A high-speed motor vehicle collision resulted in a closed transverse acetabular fracture with associated comminuted posterior wall (PW) fracture-dislocation. The femoral head exhibited impaction and comminution, with local cancellous bone crushed and the femoral head itself also sustaining compressive injury from the denser acetabular bone. Neurovascular examination was unremarkable. Initial CT imaging delineated the acetabular fracture planes, displacement, comminution of the posterior wall, femoral head impaction, and absence of soft tissue attachment to the caudal PW fragment.
Preoperative Plan
Planning remarks: The preoperative plan was for open reduction and internal fixation via a posterior approach, specifically a Kocher-Langenbeck (KL) exposure, to allow direct visualization and manipulation of the transverse fracture plane and posterior wall fragments. Percutaneous biplanar fluoroscopy-guided cannulated cancellous lag screw fixation was planned for the transverse component, with subsequent buttress plating of the posterior wall fragments.
Surgical Discussion
Patient positioning: The patient was positioned prone on a radiolucent operating table to facilitate posterior pelvic access and allow intraoperative fluoroscopic imaging in multiple planes.
Anatomical surgical approach: A Kocher-Langenbeck approach was performed: a longitudinal incision centered over the greater trochanter, with dissection through the gluteal fascia and splitting of the gluteus maximus muscle. The short external rotators were identified and detached from their femoral insertions, with care to protect the sciatic nerve. Subperiosteal elevation of the piriformis and obturator internus tendons exposed the posterior column and wall of the acetabulum. The comminuted posterior wall fragments were identified; the caudal fragment was noted to be devoid of soft tissue attachments. The transverse fracture plane was visualized, debrided, and reduced under direct vision.
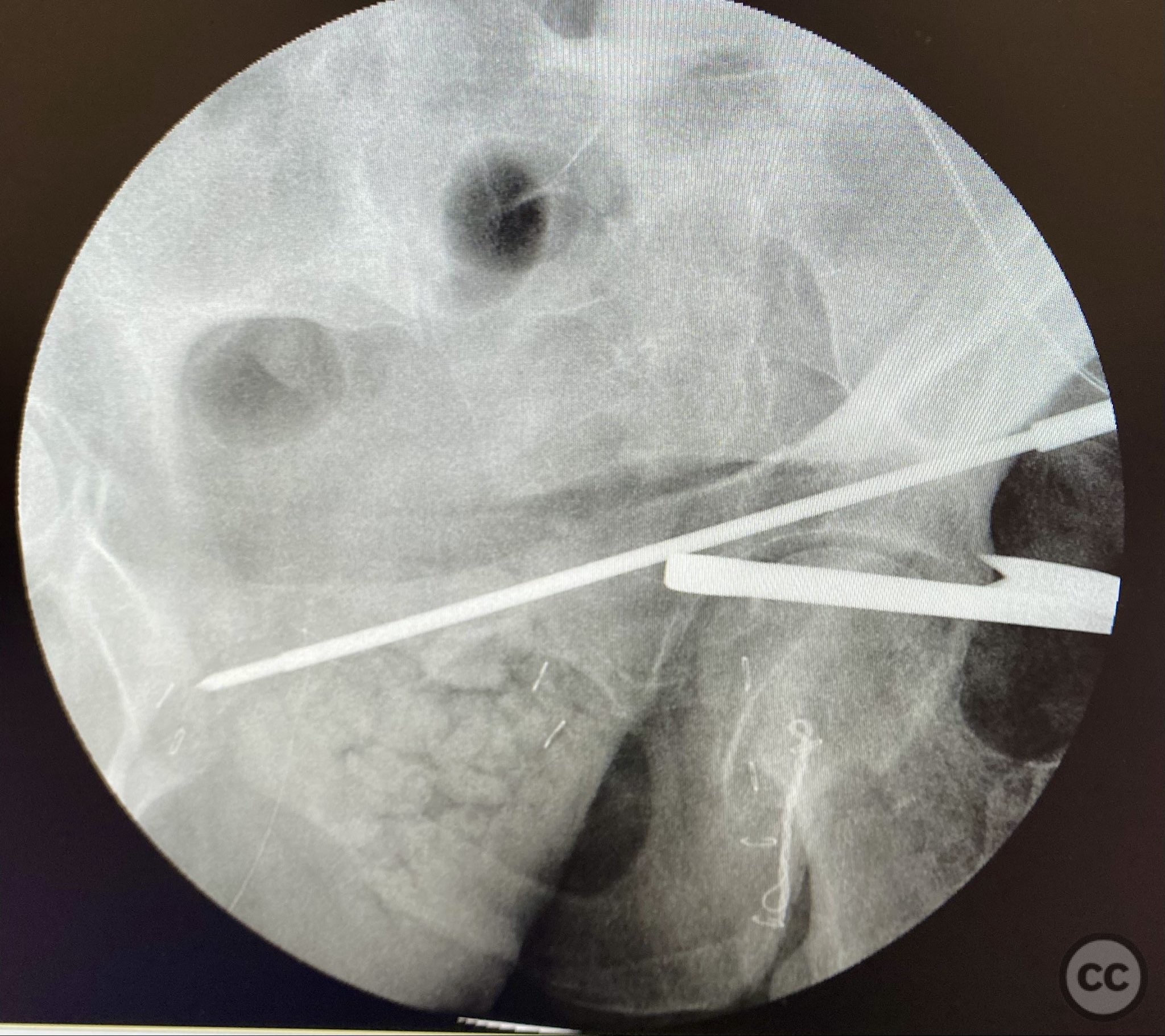
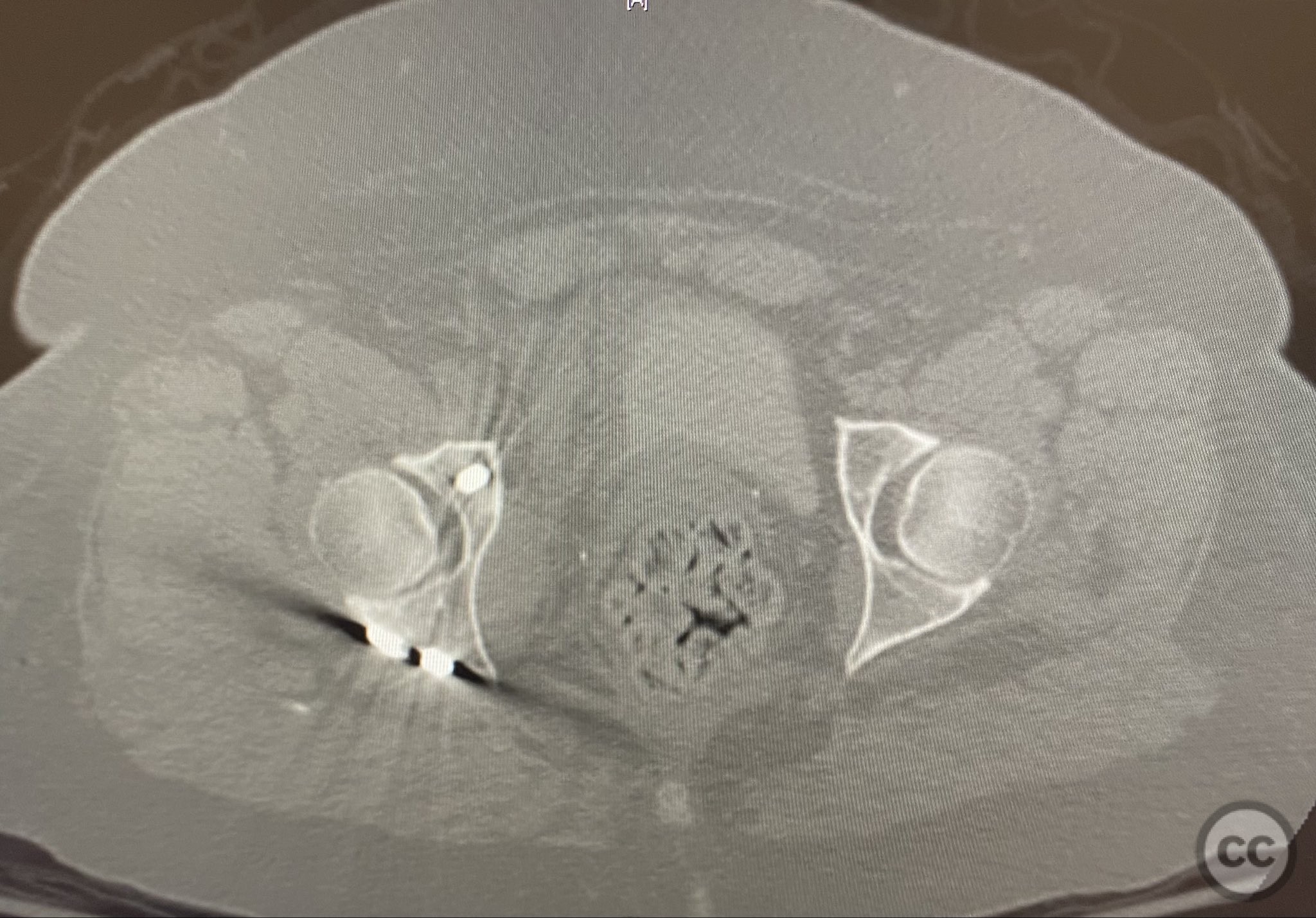
Operative remarks:The transverse fracture was manipulated and temporarily stabilized using a reduction clamp applied across the fracture plane. Under biplanar fluoroscopic guidance, a cannulated cancellous lag screw was percutaneously inserted to achieve interfragmentary compression across the transverse component. The reduction clamp was then removed. Posterior wall fragments were anatomically reduced and stabilized with contoured buttress plates spanning both the posterior wall and providing additional stabilization to the transverse component. Postoperative CT confirmed satisfactory reduction and fixation of both acetabular columns and restoration of articular congruity.
Postoperative protocol: Postoperatively, skeletal traction was discontinued. The patient was maintained non-weight bearing on the affected limb for 8 weeks, with early passive range of motion exercises initiated at 48 hours post-surgery. Progressive weight bearing was introduced after radiographic evidence of healing at 8–10 weeks.
Follow up: Not specified
Orthopaedic implants used: Cannulated cancellous lag screw; contoured acetabular buttress plates
Search for Related Literature


Industry Sponsership
contact us for advertising opportunities
Article viewed 293 times
12 Sep 2025
Add to Bookmarks
Full Citation
Cite this article:
Routt, ML. (2025). Transverse with Comminuted Posterior Wall Acetabular Fracture-Dislocation Treated by Prone Kocher-Langenbeck Approach. Journal of Orthopaedic Surgery and Traumatology. Case Report 10890414 Published Online Sep 12 2025.